The fourth suture in MACS facelifting – adressing the neck
Die vierte Naht zur Halsstraffung im MACS-Lift
Abstract
Objective:The MACS facelift alone shows poor results on the medial neck in cases of pronounced, rigid platysmabands (McKinney III–IV°).
Kai O. Kaye
1Daniel R. Sattler
2The original MACS (“Minimal Access Cranial Suspension”) facelift de- livers excellent results on the midface and leads to sustainably improved
outcome on the neck by adding a fourth suture on the platysma. 1 Oceanclinic, Plastic and Aesthetic Surgery, Marbella, Spain
McKinney type I–II platysmabands can be treated only by lateral ap- proach of the ‘fourth suture’, type III–IV should be treated with closed
platysma myotomy before. 2 University Hospital
Magdeburg, Department of Methods:Between October 2007 and November 2013 a number of
219 patients were treated with the MACS facelift technique accom- Plastic, Aesthetic and Handsurgery, Magdeburg, Germany
plished by a fourth suture on the platysma and liposuction or optional lipectomy on the neck. On 47 patients closed transcutaneous platysma myotomy was performed.
Results:Surgery time lasted on average 2.5 hours and was performed under sedation with local anesthesia in 85%. Recovery time ranged between 14 to 16 days until the patients were back to work. Due to their health status 54% of our patients had an inpatient arrangement for one night and 46% an outpatient arrangement.
Conclusion:The modification of the MACS lift with the ‘fourth suture’
on the platysma keeps the benefits of the original technique but im- proves the aesthetic outcome on the neck.
Keywords:MACS lift, face lift, neck lift, fourth suture, platysma myotomy
Zusammenfassung
Einleitung:Das MACS-Facelift alleine liefert unbefriedigende Ergebnisse im Bereich des medialen Halses, besonders wenn ausgeprägte Platys- mabänder bestehen (McKinney II–IV°). Die Erstbeschreibung des MACS- Facelift („Minimal Access Cranial Suspension“) nach Tonnard et al. er- zielt exzellente Ergebnisse im mittleren und unteren Gesichtsdrittel bis zur Mandibula. Durch eine vierte laterale Platysmanaht gelingt es auch die mediale Halsregion nachhaltig zu straffen. Weniger ausgeprägte Platysmabänder (McKinney I–II°) können allein durch den lateralen Zug der vierten Naht korrigiert werden, während akzentuierte Platysma- bänder (McKinney III–IV°) primär mit einer geschlossenen Platysma- band-Myotomie angegangen werden sollten.
Material und Methoden:Zwischen Oktober 2007 und November 2013 wurden 213 Patienten mit einem MACS-Facelift und eine zusätzliche vierte laterale Platysmanaht operiert. Die Halsregion wurde immer mit einer Liposuktion und optional mit einer offenen Lipektomie behandelt.
Bei 47 Patienten wurde eine geschlossene transkutane Platysmaband- Myotomie durchgeführt.
Ergebnisse:Die durchschnittliche Operationszeit betrug 2,5 h und 85%
der Fälle wurden unter Sedation/Lokalanästhesie operiert. Die mittlere Regenerationszeit bis zur Rückkehr in den Beruf betrug 14–16 Tage.
In Abhängigkeit der Grunderkrankungen wurden 54% der Patienten stationär, 46% ambulant geführt.
Schlussfolgerung: Die Modifizierung des MACS-Facelifts durch die vierte Naht erhält die Vorteile eines „short scar“-Faceliftes, verbessert aber nachhaltig die ästhetische Kontur des Halses.
Figure 1: Young patient requesting a facelift, pre- (a, c, e) and postoperative view (b, d, f)
Introduction
Facelifting is a crucial tool in the daily practice of a plastic surgeon. Ten to 15 years ago the facelifting procedures were requested by a small patient population in Europe [1]. Today it is widely requested and standard repertoire of every aesthetic surgeon. The request for a face lift procedure is claimed by much younger and better in- formed patients (Figure 1, Figure 2, Figure 3) [2]. This change of attitude among patients implies a challenge for the treating surgeon as these patients usually expect minimal scarring, short down time and natural results.
We introduce modifications on the MACS (“Minimal Ac- cess Cranial Suspension”) lift that accomplish these ex- pectations and provide an excellent treatment option for a large patient group.
Material and methods
Between October 2007 and January 2013 a number of 219 patients were treated with the MACS lift technique accomplished by a fourth suture on the platysma and liposuction or optional lipectomy on the neck. We found a mean age 58 years and operated on 168 female, 51 male patients. Follow-up was scheduled 1, 3, 6, 12, 24 months after surgery (Table 1). On 89 patients closed transcutaneous platysma myotomy was performed. On six patients the platysma myotomie was performed sec- ondary under local anesthesia, because they complained remaining platysmaband appearance after the primary classic MACS lift.
Surgery time lasted on average 2.5 hours and was per- formed under sedation with local anesthesia in 85%. We prefer the optional intraoperative patient mobility of the head and neck and appreciate the higher muscle tone under sedation compared to general anesthesia. Recovery time ranged between 14 to 16 days until the patients were back to work. Due to their health status 54% of our patients had an inpatient arrangement for one night and 46% an the outpatient arrangement.
In 91% the modified MACS lift was combined with other rejuvenation procedures of the face: fat grafting 1%, canthopexy 10%, perioral peeling 18%, injectables 21%, eyebrow lift 24%, platysma myotomy 35%, malar sling lift 37%, blepharoplasty superior/inferior 51%/56%, liposuc- tion neck 97%.
Modification
For cases of severe cervical excess skin and destinct platysmabands we describe a modification of the original MACS lift which maximizes the rejuvenation effect on the neck but keeps the proven benefits of short and barely visible scars. The modification consists of a fourth SMAS (“Subcutaneous Musculo Aponeurotic System”) plication suture on the lateral aspect of the platysma and a 3–4 cm advanced dissection below the mandible to accentuate the submandibular angle.
Figure 2: Young patient requesting a facelift, pre- (a, c, e) and 24 months postoperative view (b, d, f)
Figure 3: Young patient requesting a facelift, pre- (a, c, e) and 6 months postoperative view (b, d, f) Table 1: Follow up compliance of male and female patients
bilateral and adresses the medial platysma with an ad- equate lifting effect (Figure 5). Several authors support that aging leads to a certain medialisation of facial skin which is counteracted by the fourth suture on the platysma (Figure 6) [4]. The bilateral approach to correct the platysma appears more physiologically compared to a medial corsettplasty which is prone to subcutaneous visible scar formation. Hughe amounts of cervical skin can be redistributed without any tenting phenomenon on the neck (Figure 7).
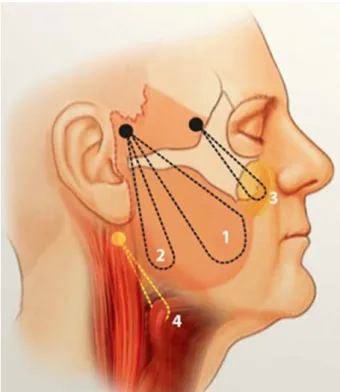
Figure 4: Traction vector of the ‘fourth suture’ (yellow) with its anchorage point on the sternocleidomastoid fascia (K. O. Kaye)
Figure 5: Standard MACS lift dissection boarders (yellow), boarders of dissection neccessary for the ‘fourth suture’
(orange), lipodissection boarders (green) and traction vector (white)
Platsyma myotomy
Platysmabands can be either soft as result of a relaxed muscle filament due to aging or hard when it forms palpable fibrotic muscle cords. Careful preoperative ex- amination disginguishes both types and indicates the adequate surgical technique.
Soft platysmabands (McKinney I–II°) can be treated with good results by the fourth suture (Figure 7). Hard platys- mabands (McKinney III–IV°) need to be treated by myotomy before applying the fourth suture [5]. We use a closed myotomy by placing serveral stab incisions (2–3 mm) along the palpable platysmaband (distance 2–3 cm). Hollow canulas are pierced through the incisions dorsal and ventral to the platysmaband. A polyfilament thread (2-0) or wire is flossed in a U-shape around the platysmaband and the canulas are removed. By moving it laterally back and forth with decent pressure, it is used like a saw to dissect the platysmaband on 4 to 5 locations (Figure 8). The technique was described by different au- thors such as Daher et al. [6], [7]. Only after platys- maband myotomy the fourth suture can evolve its full impact on medial platysma lifting.
Complications
The modification of the MACS lift through the fourth su- ture on the platysma and liposuction or optional lipectomy on the neck did not alter the complication rate compared to Verpaele et al. [3]. We analysed a complication rate of 6% which is analog to the classic MACS lift. One patient
Figure 6: Relaxed (a) and tentioned (b) ‘fourth suture’ and its impact on the medial neck
Figure 7: Illustration of the amount of cervical skin that can be redistributed during the modified MACS lift with its ‘fourth suture’
needed revision of a postoperative bleeding due to a poorly controlled hypertension. Two patients suffered from a self-limiting preauricular bleeding (<2 cm), which did not need to be revised. One patient suffered from a superficial preauricular skin necrosis (<1,5 cm) that healed by secondary intention without sequelae. One patient showed postoperative neurapraxy of the marginial mandibular branch of the facial nerve that recovered without sequelae within 2 months. There were no injuries of the zygomatic or buccal branches of the facial nerve.
Discussion
The MACS facelift technique was described by Tonnard and Verpaele and evolved to an established and popular technique for facial rejuvenation [3], [8], [9], [10]. The main advantages of the method are highlighted: Short, barely visible scars, which make the procedure attractive for many patients especially for male patients or female patients with short hair. Limited undermining decreases the risk of blood circulation disorders and skin necrosis particularly in patients at risk, such as smokers. The technique is less invasive than most SMAS (“Subcu- taneous Musculo Aponeurotic System”) elevation or SMAS dissection techniques. It is a save procedure in relation
Figure 8: Outcome of a modified MACS lift and the ‘fourth suture’, pre- (a, c, e) and 6 months postoperative view (b, d, f) to potential nerve injuries and has a shorter postoperative
down time [11].
Due to the short scar and the purely vertical lifting vector the option to redistribute larger amounts of excess skin of the medial neck and submandibular area is limited [10]. Redistribution of skin is prone to leave pleats the preauricular area resulting in uneven perilobular scars.
The MACS lift alone shows poor results on the medial neck in cases of pronounced, rigid platysmabands (McKinney III–IV°) [10], [12].
The strictly vertical lifting vector as described in the ori- ginal publication does not sufficiently adress the platysma and fails to correct medial platysmabands. Since the vertical traction on the platysma originates cephalad of the ramus mandibulae a tenting phenomenon results (Figure 9). The platysma spans and raises the underlying submandibular fat in a convex instead concave way. As a result the cervicomandibular angle is blurred instead of defined.
Verpaeles et al. original publication recognizes the first two disadvantages and recommends a combination of their technique with an anterior cervicoplasty to correct medial platysmabands and a posterior cervicoplasty to prevent lateral skin pleats in the preauricular area [9].
The presumption of Verpaele et al. that extended dissec- tion along the platysma would lead to a higher rate of postoperative bleedings could not be seen in our patients.
All surgeries were done under perioperative epinephrine application. Since the duration of action is shorter than surgery time we found no altered risk of delayed reactive hyperemia and consecutive postoperative bleeding. The use of perioperative epinephrine administration facilitates the identification of functional structures, allows safer dissection and shortens surgery time [13]. Analgosedation provides physiologic blood pressure throughout the sur- gery without reactive alterations especially during extuba- tion [14]. After facial liposuction the dissection of the very delicate facial flaps should be performed carefully, any
pressure or stretching of the flap should be avoided. On smokers limited undermining can be indicated to prevent necrosis [15], [16]. Plication techniques of the SMAS are less prone to nerve injuries compared to smasectomy methods [17].
Conclusion
The modification of the MACS lift with the ‘fourth suture’
on the platysma keeps the benefits of the original tech- nique but improves the aesthetic outcome on the neck (Figure 10). Short scars, short surgery time and a high safty of the procedure make it convenient to both patient and surgeon. Platysmabands should be examined and classified prior to surgery. McKinney type I–II can be treated only by lateral approach of the ‘fourth suture’, type III-IV should be treated with closed platysma myotomy before. Liposuction of the cheeks and neck is an import- ant tool to prepare and ease dissection. Optional retro- platysma lipectomy can be indicated to reconstruct the cervico-mandibular angle if retroplatysma fat deposits are responsible for a hanging neck. The original technique of the MACS lift delivers excellent results on the midface and leads to sustainably improved outcome by adding the fourth suture as key procedure to accentuate the mandibular angle of the neck.
Figure 9: Closed myotomy of hard platysma bands (McKinney III–IV°)
Figure 10: Disappearance of hard platysma bands (McKinney III–IV°) after closed myotomy, modified MACS lift and the ‘fourth suture’
1. Friel MT, Shaw RE, Trovato MJ, Owsley JQ. The measure of face- lift patient satisfaction: the Owsley Facelift Satisfaction Survey with a long-term follow-up study. Plast Reconstr Surg. 2010 Jul;126(1):245-57. DOI: 10.1097/PRS.0b013e3181dbc2f0 2. Pusic AL, Klassen AF, Scott AM, Cano SJ. Discussion. The
measure of face-lift patient satisfaction: the Owsley Facelift Satisfaction Survey with a long-term follow-up study. Plast Reconstr Surg. 2010 Jul;126(1):258-60. DOI:
10.1097/PRS.0b013e3181dbba19
3. Verpaele A, Tonnard P, Gaia S, Guerao FP, Pirayesh A. The third suture in MACS-lifting: making midface-lifting simple and safe.
J Plast Reconstr Aesthet Surg. 2007;60(12):1287-95. DOI:
10.1016/j.bjps.2006.12.012
4. Truswell WH 4th. Aging changes of the periorbita, cheeks, and midface. Facial Plast Surg. 2013 Feb;29(1):3-12. DOI:
10.1055/s-0033-1333840
5. McKinney P. The management of platysma bands. Plast Reconstr Surg. 1996 Nov;98(6):999-1006. DOI: 10.1097/00006534- 199611000-00011
6. Daher JC. Closed platysmotomy: a new procedure for the treatment of platysma bands without skin dissection. Aesthetic Plast Surg. 2011 Oct;35(5):866-77. DOI: 10.1007/s00266-011- 9782-0
7. Gonzalez R. Composite platysmaplasty and closed percutaneous platysma myotomy: a simple way to treat deformities of the neck caused by aging. Aesthet Surg J. 2009 Sep-Oct;29(5):344-54.
DOI: 10.1016/j.asj.2009.04.007
8. Tonnard P, Verpaele A. The MACS-lift short scar rhytidectomy.
Aesthet Surg J. 2007 Mar-Apr;27(2):188-98. DOI:
10.1016/j.asj.2007.01.008
9. Tonnard PL, Verpaele A, Gaia S. Optimising results from minimal access cranial suspension lifting (MACS-lift). Aesthetic Plast Surg.
2005 Jul-Aug;29(4):213-20; discussion 221. DOI:
10.1007/s00266-005-0047-7
10. Verpaele A, Tonnard P. Lower third of the face: indications and limitations of the minimal access cranial suspension lift. Clin Plast Surg. 2008 Oct;35(4):645-59, vii. DOI:
10.1016/j.cps.2008.04.001
Nov;17(4):531-8, v. DOI: 10.1016/j.fsc.2009.06.010 15. Abboushi N, Yezhelyev M, Symbas J, Nahai F. Facelift
complications and the risk of venous thromboembolism: a single center’s experience. Aesthet Surg J. 2012 May;32(4):413-20.
DOI: 10.1177/1090820X12442213
16. Knobloch K, Gohritz A, Reuss E, Vogt PM. Nikotinkonsum und plastische Chirurgie: Eine aktuelle Ubersicht [Nicotine in plastic surgery: a review]. Chirurg. 2008 Oct;79(10):956-62. DOI:
10.1007/s00104-008-1561-3
17. Prado A, Andrades P, Danilla S, Castillo P, Leniz P. A clinical retrospective study comparing two short-scar face lifts: minimal access cranial suspension versus lateral SMASectomy. Plast Reconstr Surg. 2006 Apr;117(5):1413-25; discussion 1426-7.
DOI: 10.1097/01.prs.0000207402.53411.1e
Corresponding author:
Dr. med. Daniel R. Sattler
University Hospital Magdeburg, Department of Plastic Aesthetic and Handsurgery, Leipziger Str. 44, 39120 Magdeburg, Germany
daniel@sattler.com
Please cite as
Kaye KO, Sattler DR. The fourth suture in MACS facelifting – adressing the neck. GMS Ger Plast Reconstr Aesthet Surg. 2014;4:Doc09.
DOI: 10.3205/gpras000028, URN: urn:nbn:de:0183-gpras0000286
This article is freely available from
http://www.egms.de/en/journals/gpras/2014-4/gpras000028.shtml Published:2014-12-22
Copyright
©2014 Kaye et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by-nc-nd/3.0/deed.en). You are free: to Share — to copy, distribute and transmit the work, provided the original author and source are credited.