Technical tip: Side-to-side tendon suture as escape plan during extensor indicis tendon plasty in distal extensor pollicis longus rupture
Technik-Tip: Seit-zu-Seit-Sehnennaht als chirurgischer Ausweg zur Extensor indicis-Plastik bei distaler Ruptur der Extensor pollicis longus-Sehne
Abstract
Objective:In case of a short distal recipient stump after extensor pollicis longus (EPL) tendon rupture, transfer of the extensor indicis proprius
Andrea Christina Schleh
1(EIP) tendon using a conventional Pulvertaft tendon-weaving technique
Andreas Gohritz
1may be difficult or impossible. The purpose of this paper is to provide
Beate Wilmink
2a technical tip to manage this rare, but clinically important scenario of
a very short distal EPL recipient tendon.
Jan Fridén
3Methods:A side-to-side tendon suture (SSTS) was used for EIP transfer
to restore thumb extension in 3 patients who had sustained a distal
Dirk J. Schaefer
1rupture of their extensor pollicis longus near the interphalangeal joint.
The SSTS was performed with an overlap of 2 cm in 2 patients and 2.5 cm in one patient.
1 Plastische, Rekonstruktive, Ästhetische Chirurgie und Results:A stable SSTS was achieved which allowed early active mobil-
ization and resulted in good functional recovery of thumb extension after a mean follow-up of 8 months.
Handchirurgie,
Universitätsspital Basel, Schweiz
Conclusion:Extensor indicis transfer using SSTS is a reliable and tech- nically simple escape plan in a distal rupture of the EPL near the
2 Klinik für Handchirurgie, Bad Neustadt a.d. Saale, Deutschland interphalangeal joint. It provides very stable tendon-to-tendon attach-
ment with high loading capacity and good gliding qualities. 3 Schweizer Paraplegiker- Zentrum, Nottwil, Schweiz Keywords:technical tip, side-to-side tendon suture, Pulvertaft, weaving,
immediate mobilization
Zusammenfassung
Ziel:Die herkömmliche Sehnenverflechtungsnaht nach Pulvertaft zur Extensor indicis-Sehnentransposition nach Ruptur der Extensor pollicis longus-Sehne ist bei kurzen Stümpfen technisch schwierig oder unmög- lich. Dieser Beitrag gibt einen Technik-Tip, wie in dieser seltenen, aber klinisch relevanten Situation bei sehr kurzer distaler EPL-Sehne vorge- gangen werden kann.
Methoden:Eine Seit-zu-Seit-Sehnennaht (SSSN) wurde bei 3 Patienten zur Extensor indicis-Verlagerung bei Ruptur der Extensor pollicis longus- Sehne nahe dem IP-Gelenk des Daumens verwendet. Diese Nahttechnik wurde mit einer Überlappung von 2 cm in 2 Patienten und einmal von 2,5 cm durchgeführt.
Ergebnisse:Es konnte eine stabile SSSN erreicht werden, die eine frühe aktive Nachbehandlung und nach einer mittleren Nachbeobachtungszeit von 8 Monaten eine gute Funktionswiederherstellung der Daumen- extension ermöglichte.
Schlussfolgerung:Die EIP-Transposition mittels SSSN ist ein zuverlässi- ger chirurgischer Ausweg bei Ruptur der EPL-Sehne nahe des Daumen- endgelenks. Sie bietet eine stabile Sehnenvereinigung mit hoher Belas- tungsfähigkeit und guter Sehnengleitfähigkeit.
1/4 GMS German Plastic, Reconstructive and Aesthetic Surgery 2015, Vol. 5, ISSN 2193-7052
Research Article
OPEN ACCESS
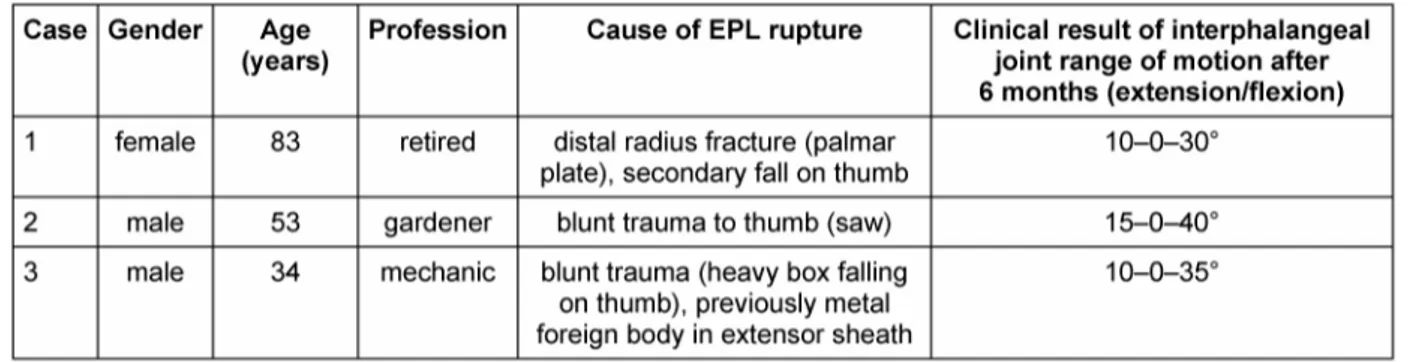
Table 1: Patient characteristics and clinical results
Introduction
If rupture of the EPL tendon occurs close to the interphalangeal joint of the thumb resulting in a short distally remaining tendon stump, a conventional braiding suture according to Pulvertaft may be difficult if not im- possible. A side-to-side tendon suture may be a valuable alternative.
Methods
Operative Technique
The SSTS was performed under local anaesthesia (Rapidocain 1%, with Epinephrin 1:100,000). The EIP donor tendon was laid onto the short recipient tendon stump of the EPL and both tendon were united with a test suture. The tension of the transfer was adjusted using active cooperation of the (“wide awake”) patient using the tenodesis effect during wrist flexion (extension of the thumb IP joint) and extension (flexion of the thumb and contact of its tip to the lateral index finger). The perman- ent suture was then performed by a back and forth crossed running suture on both sides of the 2 tendons (4-0 Prolene). In one patient, the extensor hood of the very short recipient tendon was also partly included.
Postoperativey, hand therapy was started on the 1stpostoperative day. Unloaded thumb interphalangeal flexion and extension was allowed immediately during exercises. The patient wore an abduction splint between exercises for the first 3 weeks, then the splint was re- moved in daily life and only worn during special load until 6 weeks postoperatively.
Patients
During an 8-months-period, 3 patients (1 female, 2 males) with a mean age of 57 years presented to our hand sur- gery clinic due to a traumatic rupture of the EPL distal to the Listers tubercle with a recipient tendon stump of less than 3 centimetres. The cause of this atypical EPL rupture with a very short distal end was once a distal tendon degeneration after plate osteosynthesis of distal radius fracture and in 2 patients a distal blunt trauma, in one case with a metal foreign body in the extensor pollicis longus tendon sheath due to previous trauma. The SSTS was performed with an overlap of 2 cm in 2 patients and 2.5 cm in one patient.
Results
In all 3 patients a stable tendon attachment was accom- plished despite a short distal end of EPL tendon. Early functional exercising under splint protection was possible starting on the first postoperative day. A good functional result with full active extension of the thumb interphalan- geal joint beyond neutral could be achieved in all cases after a mean follow-up of 8 months (range 6–10, min- imum of 6 months) (Table 1).
Case description
A 34-year-old male had sustained an explosion trauma to his left hand 5 years ago with entrapment of a metal foreign body in the extensor pollicis longus tendon sheath of the left thumb. After additional blunt trauma due to a heavy box falling onto his left thumb he presented with an EPL-tendon rupture shortly proximal to the left inter- phalangeal joint (Figure 1). He underwent reconstruction by extensor indicis tendon transfer using a SSTS with a 2 cm overlap (Figure 2). At the follow-up examination 6 months postoperatively, he achieved active range of motion of the left IP joint of extension/flexion 10–0–35°
(right side 20–0–60°). He recovered left hand grasp of 49 kg (right side 53 kg) and thumb-index pinch of 10 kg (right side 11 kg) (Figure 3) and has resumed his job as a mechanic.
2/4 GMS German Plastic, Reconstructive and Aesthetic Surgery 2015, Vol. 5, ISSN 2193-7052
Schleh et al.: Technical tip: Side-to-side tendon suture as escape ...
Figure 1: Distal EPL rupture with a short (2.5 cm) distal tendon stump
Figure 2: Restoration of thumb extension by extensor indicis proprius tendon transfer using SSTS technique
Figure 3: Functional recovery of EPL function 6 months postoperatively
Discussion
Rupture of the EPL tendon mostly occurs after distal radius or scaphoid fractures, tenosynovialitis, steroid in- jections or misplaced external fixator or K-wires for osteo- synthesis. The underlying mechanism apparently is inter- ruption of the tendon’s vascularity due to haematoma and pressure making the damaged tendon more suscept- ible to rupture due to secondary ischemic degeneration and necrosis. Usually, the rupture occurs just distal to the extensor retinaculum where the EPL turns around the roughened Lister’s tubercle. Most commonly tendon transfer is indicated [1]. However, if the EPL ruptures distally, the short recipient stump may prevent a conven- tional weaving technique [2] and any hand surgeon should have a surgical life-boat when confronted with this scenario. Furthermore, multiple studies have shown that early passive and active mobilization and guided loading of a transferred muscle improves joint range of motion and increases vascularity and tensile strength [3], [4], [5]. A strong surgical repair is required to allow early ac- tivation of a transferred muscle and load the repair with a minimum risk of damaging the suture site [6]. The SSTS has been designed to function as a repair that permits immediate postoperative activation and mobilization of a transferred muscle. It is technically easy and performed on both sides using back and forth crossed-stitches [7].
It has been proven to be highly stable and even stronger than Pulvertaft, allowing immediate exercise with a load limit of 200 N, which means a safety factor 10–20 times higher than the expected load during guided exercise [8].
The SSTS is used widely in tendon transfers, e.g. in functional reconstructions in tetraplegia where immediate mobilization may prevent adhesions and provide more rapid recovery of function. Generally, an overlap of 5 cm is recommended [9]. This was not possible in our specific patient series imposed by the short distal recipient EPL tendon stump. However, thumb extension does not re- quire high force and a shorter contact length of the donor and recipient tendons was obviously sufficient to allow immediate postoperative training and achieve a good functional result. This study is limited by the small patient
3/4 GMS German Plastic, Reconstructive and Aesthetic Surgery 2015, Vol. 5, ISSN 2193-7052
Schleh et al.: Technical tip: Side-to-side tendon suture as escape ...
number due to the rare occurence of EPL rupture distally to the classic location near Listers tubercle. However, EIP-to-EPL transfer is a well-established procedure with good short- and long-term results already documented [10], [11], [12]. The main objective of this paper was to draw attention to a technical modification in an exception- al, but clinically important situation. The utilized STSS offers a technically easy and reliable alternative to the Pulvertaft tendon weaving suture also in all other kinds of tendon transfers.
Conclusions
The SSTS is a reliable and technically simple procedure, which provides very stable tendon-to-tendon attachment with high loading capacity and good gliding qualities. It is especially useful if only a short overlap of donor and recipient tendon is feasible, such in very distal EPL tendon rupture. It has become a valuable alternative to the formerly Pulvertaft tendon weaving suture in a variety of tendon transfers in our practice.
Notes
Competing interests
The authors declare that they have no competing in- terests.
References
1. Gelb RI. Tendon transfer for rupture of the extensor pollicis longus. Hand Clin. 1995 Aug;11(3):411-22.
2. Pulvertaft RG. Tendon grafts for flexor tendon injuries in the fingers and thumb; a study of technique and results. J Bone Joint Surg Br. 1956 Feb;38-B(1):175-94.
3. Gelberman RH, Woo SL, Lothringer K, Akeson WH, Amiel D.
Effects of early intermittent passive mobilization on healing canine flexor tendons. J Hand Surg Am. 1982 Mar;7(2):170-5.
DOI: 10.1016/S0363-5023(82)80083-X
4. Rath S. Immediate active mobilization versus immobilization for opposition tendon transfer in the hand. J Hand Surg Am. 2006 May-Jun;31(5):754-9. DOI: 10.1016/j.jhsa.2006.01.018 5. Gelberman RH, Amifl D, Gonsalves M, Woo S, Akeson WH. The
influence of protected passive mobilization on the healing of flexor tendons: a biochemical and microangiographic study.
Hand. 1981 Jun;13(2):120-8. DOI: 10.1016/S0072- 968X(81)80051-4
6. Rath S. Immediate postoperative active mobilization versus immobilization following tendon transfer for claw deformity correction in the hand. J Hand Surg Am. 2008 Feb;33(2):232- 40. DOI: 10.1016/j.jhsa.2007.10.012
7. Fridén J, Reinholdt C. Current concepts in reconstruction of hand function in tetraplegia. Scand J Surg. 2008;97(4):341-6.
8. Brown SH, Hentzen ER, Kwan A, Ward SR, Fridén J, Lieber RL.
Mechanical strength of the side-to-side versus Pulvertaft weave tendon repair. J Hand Surg Am. 2010 Apr;35(4):540-5. DOI:
10.1016/j.jhsa.2010.01.009
9. Reinholdt C, Fridén J. Outcomes of single-stage grip-release reconstruction in tetraplegia. J Hand Surg Am. 2013 Jun;38(6):1137-44. DOI: 10.1016/j.jhsa.2013.02.041 10. Hoch J, Lösch GM, Schrader M. Langzeitresultate nach
Rekonstruktion der Sehne des M. extensor pollicis longus durch Transposition der Sehne des M. extensor indicis [Long-term results following reconstruction of the tendon of the extensor pollicis longus muscle by transposition of the tendon of the extensor indicis muscle]. Handchir Mikrochir Plast Chir. 1988 Mar;20(2):93-6.
11. Giessler GA, Przybilski M, Germann G, Sauerbier M, Megerle K.
Early free active versus dynamic extension splinting after extensor indicis proprius tendon transfer to restore thumb extension: a prospective randomized study. J Hand Surg Am. 2008 Jul- Aug;33(6):864-8. DOI: 10.1016/j.jhsa.2008.01.028 12. Lalonde DH. Wide-awake extensor indicis proprius to extensor
pollicis longus tendon transfer. J Hand Surg Am. 2014 Nov;39(11):2297-9. DOI: 10.1016/j.jhsa.2014.08.024
Corresponding author:
Dr. med. Andrea Christina Schleh
Plastische, Rekonstruktive, Ästhetische Chirurgie und Handchirurgie, Universitätsspital Basel, Spitalstrasse 21, 4031 Basel, Schweiz
Andrea.schleh@usb.ch
Please cite as
Schleh AC, Gohritz A, Wilmink B, Fridén J, Schaefer DJ. Technical tip:
Side-to-side tendon suture as escape plan during extensor indicis tendon plasty in distal extensor pollicis longus rupture. GMS Ger Plast Reconstr Aesthet Surg. 2015;5:Doc07.
DOI: 10.3205/gpras000035, URN: urn:nbn:de:0183-gpras0000355
This article is freely available from
http://www.egms.de/en/journals/gpras/2015-5/gpras000035.shtml Published:2015-11-03
Copyright
©2015 Schleh et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 License. See license information at http://creativecommons.org/licenses/by/4.0/.
4/4 GMS German Plastic, Reconstructive and Aesthetic Surgery 2015, Vol. 5, ISSN 2193-7052
Schleh et al.: Technical tip: Side-to-side tendon suture as escape ...