Determinants of neonatal and under-three mortality in Central Asian countries: Kyrgyzstan, Kazakhstan and Uzbekistan Determinanten der
Kindersterblichkeit in der
neonatalen Periode und in den drei ersten Lebensjahren in drei Ländern Zentralasiens:
Kirgisistan, Kasachstan and Usbekistan
• Manas K. Akmatov1• Rafael T. Mikolajczyk1• Alexander Krämer1
Hintergrund: Unterschiedliche Studien untersuchten Faktoren, die mit der Kinder- sterblichkeit insbesondere in Entwicklungsländern assoziiert waren, wenig bekannt ist aber über die früheren kommunistischen Länder. Wir untersuchten deshalb, welche Faktoren die Kindersterblichkeitsraten in den zentralasiatischen Ländern Kirgisistan, Kasachstan and Usbekistan beeinflussten. Zwei Aspekte waren von besonderem Interesse, der Einfluss des Wohnortes (Land gegenüber Stadt) auf das Sterblichkeits- risiko und die Altersabhängigkeit (neonatale Mortalität gegenüber Kindersterblichkeit in den drei ersten Lebensjahren).
Methoden: Wir benutzten die Datensätze der Demographic and Health Surveys in den drei zentralasiatischen Ländern. Der kombinierte Datensatz beinhaltete Information über 2867 Kinder bis zum Alter von drei Jahren, wovon 135 starben. Wir untersuchten drei separate multiple logistische Regressionsmodelle: für den gesamten Datensatz mit allen Kindern bis einschließlich zum dritten Lebensjahr, für neonatale Mortalität im ersten Lebensmonat und für die Sterblichkeit im 2.-36. Lebensmonat.
Ergebnisse: Die Kindersterblichkeit in den ersten drei Lebensjahren war unabhängig assoziiert mit dem Wohnen auf dem Land gegenüber dem Wohnen in der Stadt (OR 1,69 (CI 95% 1,11-2,56)), der Geburtenreihenfolge unter den Geschwistern und dem Familienstatus der Mutter (verheiratet gegenüber nicht verheiratet) (OR 0,52 (CI 0,25- 1,08)). Wohnen auf dem Land war stärker assoziiert mit Kindersterblichkeit im 2. bis zum 36. Lebensmonat als mit der neonatalen Mortalität. Die Unterschiede zwischen
1Department of Public Health Medicine, School of Public Health, University of Bielefeld, Bielefeld, Germany
OriginalArticle
den Ländern hatten hingegen einen stärkeren Einfluss auf die neonatale Mortalität als die Mortalität zwischen dem 2. und 36. Lebensmonat.
Schlussfolgerungen: Die Stadt-Land-Unterschiede im Hinblick auf die Kindersterb- lichkeit in den drei Ländern persistieren nach Adjustierung für mehrere sozioökonomi- sche Kovariaten.
Schlüsselwörter:Kindersterblichkeit, neonatale Mortalität, sozioökonomische Faktoren, Zentralasien
Objective: Several studies dealt with factors associated with childhood mortality, especially in developing countries, but less is known about former communistic countries. We therefore analyzed the factors affecting mortality rates among children in the Central Asian countries Kyrgyzstan, Kazakhstan and Uzbekistan. We focused on the impact of living place (rural versus urban) and age dependency (neonatal versus under-three mortality) on the mortality risk.
Methods: We used the Demographic and Health Surveys data (DHS) for the three Central Asian countries. The combined data set included information about 2867 children under the age of three, 135 of whom died. We studied three multiple logistic regression models: for the mortality under the age of three, for neonatal mortality (1st month of life) and for mortality in 2nd-36thmonth of life.
Results: Under-three mortality was independently associated with living in a rural versus urban area (OR 1.69 (CI 1.11-2.56)), birth order and mother not being currently married vs. married (OR 0.52 (CI 0.25-1.08)). There was a lower risk of mortality for children living in larger families (six or more household members vs. less than six, OR 0.45 (CI 0.30-0.65)). Living in a rural area was more strongly associated with mortality in 2-36 month of life than with neonatal mortality. Differences between countries were greater in neonatal mortality than in mortality between 2nd-36thmonth of life.
Conclusions: This study suggests that urban-rural differences with respect to child- hood mortality in these countries persist after adjusting for several socioeconomic factors.
Keywords:under-three mortality, neonatal mortality, socioeconomic factors, Central Asia
Introduction
Child mortality is a measure of the nation's health and worldwide indicator of social well-being. There are numerous studies that recognized maternal, socioeco- nomic, environmental and behavioral factors as import- ant determinants of child mortality, but there is a lack of information about the association between childhood mortality and different factors in the Central Asian countries [1]. Compared with most developing coun- tries, child mortality rates in the Central Asian countries are substantially lower, but still remain relatively high compared to most developed countries [2]. Further, studies in many developing countries found higher mortality rates in rural than urban areas, with a risk excess of 24% to 70% for childhood mortality [3], [4],
[5]. There are considerable differences between urban and rural areas in availability of health resources, ac- cess to education and living conditions, which may explain the higher mortality. However, higher mortality in urban areas was also observed [6]. Because of its past history in the Soviet Union all the three countries of Central Asia may have a better developed public health system with a better coverage of rural areas but share other features with developing countries.
Given the particular status of post-communistic coun- tries as compared to developing countries on the one side and developed countries on the other analyzing the determinants of mortality is of special interest. We therefore performed an analysis of reproductive health and socioeconomic factors which may affect the mor- tality rates among children in the Central Asian coun-
OriginalArticle
tries Kyrgyzstan, Kazakhstan and Uzbekistan. We in- vestigated in which way mortality rates differ between rural and urban areas in these countries. Further, we studied which factors are associated with neonatal (1st month of life) and later childhood mortality (2-36 months) and how they differ. Previous research sug- gested differences in determinants of childhood mor- tality for different age groups [7], [8].
Material and methods
We performed a secondary analysis of data collected during Demographic and Health Surveys in three Central Asian countries: Kyrgyzstan (KRDHS, 1997), Uzbekistan (UDHS, 1996) and Kazakhstan (KDHS, 1995) The datasets were provided by Macro Interna- tional [9]. All DHS surveys use a standardized ques- tionnaire with the same methodology to estimate health and other socioeconomic indicators across countries and over time. All three surveys in the Central Asian countries were national in scope and included about 4000 women each. In the urban areas the sampling unit was uchastok, which was divided into smaller segments. In the rural areas the sampling unit was the village, which also was divided into smaller segments, and only one segment was selected for the survey. A list of all households in each selected segments was prepared and households for interviews were randomly selected. The response rate was over 97% in all three countries. The surveys collected birth history data from 12,034 women aged 15-49 years, with more detailed information collected for births that occurred in the last 3 years preceding the surveys. To minimize recall bias and time effects we restricted our analysis only to mothers with children born in the latter period, resulting in a final sample size of 2867. In all three surveys a live birth was defined according to the WHO definition, i.e. a life birth is, when the child after separation from the mother breaths or shows any other signs of life, irrespective of the duration of pregnancy. This defini- tion was explained to the mother during the interview ([10], page 93). For each child the birthday and living status at the moment of interview and for children who died the age at death in months was recorded. Main findings from the surveys as well as the questionnaires are described in original reports [10], [11], [12].
We developed a joint model for the three countries under the assumptions that the Central Asian countries have similar political, demographic and socio-economic situations; the surveys were also performed over a relatively short period of time in all the countries. The assumption of a joint model was further supported by the absence of a significant interaction between country and other variables in the analysis. We ana- lyzed three separate logistic regression models where
the binary outcome variable was whether the child had died within the 36 months after birth or no (under-three mortality), the child had died in the first month of life or no (neonatal mortality) and the child had died after the first month but within 36 months of life. In all ana- lyses we used the same control group consisting of all children born during the last three years and alive at the time of the interview.
Outcomes in siblings are potentially correlated because siblings share the same risks associated with the home environment and common genetic inheritance [13].
Including several children from the same household in the analysis may lead to underestimation of the standard errors. To avoid problems with clustering of the data we therefore included in the analysis only one child per household. In the households with several children we included only the child who died, otherwise the youngest child.
The selection of potential predictors of mortality was based on a literature review [5], [14], [15], [16]. The independent variables used in the analysis refer to different factors, namely socio-economic factors (ma- ternal education, maternal and paternal occupation, the number of household members, marital status of the mother), bio-demographic factors (maternal age at first marriage, maternal age at first birth, birth order, length of the preceding birth interval, gender of the child), reproductive healthcare behavior (place of de- livery), living conditions (access to safe water), cultural characteristics (religion) and place of residence. An- other known predictor of childhood mortality - breast- feeding - was not included in the analysis because in the Central Asian countries over 95% of women are breastfeeding. This resulted in a quasi complete sep- aration in the estimation procedure. Additionally, the absence of breastfeeding in the neonatal period may not have contributed to the death by itself, but may be a result of conditions leading to the death, especially in the case of neonatal mortality [15].
Place of residence was classified into two categories:
rural areas and urban areas. Urban areas included large cities (capital cities and cities with a population over 1 million), small cities (population over 50,000) and towns (other urban areas; an exact definition was not provided in the dataset). All other areas are as- sumed to be rural areas. Two educational categories were defined for the mother: a low level, which includes no education, primary(six years),secondary education (eleven years) and a high level (university degree).
Most of the women in the low category had secondary level education. We used the occupation status of both parents as an indicator of the social status of the family. We defined two categories: those who had work and those without work. The original variablesource
OriginalArticle
of drinking waterconsisted of different categories; this variable was recoded into a binary variable: having access to safe water or no. Two categories were built for the variablethe length of the preceding birth inter- val: short intervals with less than 18 months and inter- vals longer than 18 months. Children born in first order were included into the latter group. All variables used in this analysis had nearly complete responses with less than 5% missing values. Data from all three countries were merged and the variablecountrywas included in the model.
We assessed the multicollinearity of the predictors using standard methods described in ([17], page 48).
We analyzed effects of each variable of interest using simple logistic regression (crude estimated effects).
Then we applied multiple logistic regression analysis for the analysis of independent associations. We first restricted the number of independent variables in the model to 15 to achieve a sufficient ratio of about 10 events per variable. Then we used the forward selec- tion procedure with a significance level of 0.5 for the Wald statistic as proposed by Steyerberg [18]. All po- tential interactions were included one by one in the fi- nal main effect model as proposed by Hosmer and Lemeshow [19], but none appeared significant. We used the final set of variables from the under-three mortality and analyzed the outcome with respect to neonatal mortality and mortality from 2nd-36thmonth of life. The Hosmer-Lemeshow goodness-of-fit statistic and ROC curves were used to assess the model fit and discriminative power of the model. Data analysis was conducted using statistical package SAS version 8.02.
Results
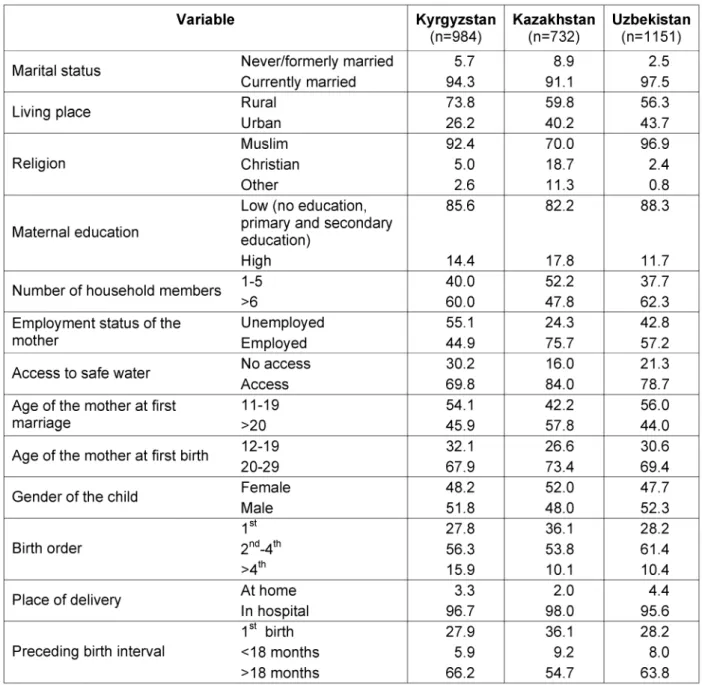
The three countries displayed similarities in several characteristics potentially associated with childhood mortality (Table 1). Over 90% of the respondents were married, the majority was living in rural areas, over 90% were Muslim (but only 70% in Kazakhstan), about half of the households had less than 6 members, between 24% and 55% were unemployed, 16% to 30% had no access to safe water.
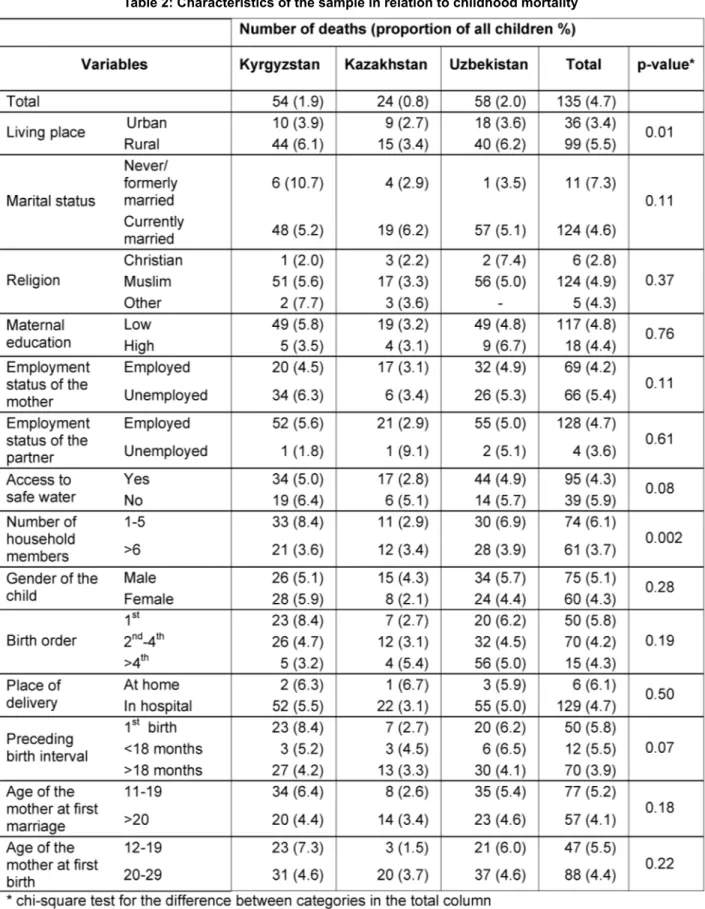
135 children died under the age of three, 67 within the first month of life and 68 after the first month but under the age of three; there were 2732 living children under age of three who were included as controls in the analysis. Table 2 shows the characteristics of the sample in relation to childhood mortality.
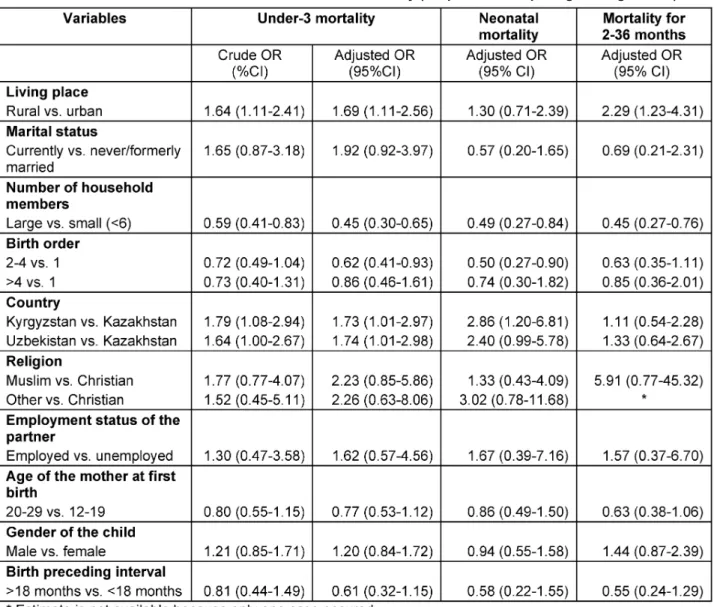
Of the 15 potential predictors of under-three mortality originally included in the model, 10 were selected for the final model (Table 3). The five strongest predictors of under-three mortality were living place, marital status
of the mother, number of household members, birth order and the country variable.
The estimate of risk associated with living in a rural area, as compared to urban, only slightly changed from simple to multiple regression models, showing that the risk excess is independent from other covari- ates included in the final model. After adjusting for other factors the benefit of living in a larger household slightly increased. The under-three mortality was about 70% higher in Kyrgyzstan or Uzbekistan versus Kazakhstan, even after adjustment for other variables.
Most of the determinants of under-three mortality did not differ between neonatal and later childhood mortal- ity, except the place of residence (urban vs. rural) and country (Kyrgyzstan and Uzbekistan vs. Kazakhstan) (Table 3, right side). The effect of place of residence was stronger for the period of 2-36 months. In contrary, the effect of living in Kyrgyzstan or Uzbekistan versus Kazakhstan was stronger for the neonatal mortality and the country-effect disappeared for the mortality of 2-36 months.
The selected set of variables performed better in pre- dicting mortality in 2-36 months of life than neonatal or under-three mortality (the area under the ROC was 0.65 for neonatal, 0.70 for later childhood and 0.66 for under-three mortality).
Discussion
We analyzed several demographic and socioeconomic predictors associated with under-three mortality in the Central Asian countries. The association with child birth order was described in the literature as an import- ant predictor of child mortality [20]. Our finding is compatible with some previous studies, where it has been shown that mortality by birth order has a U- shaped form with higher mortality among early and late birth orders. We observed a higher mortality risk for children whose mothers were currently not married.
As in many developing countries marriage in the Central Asian countries gives women security and social support, which is likely to be associated with better childhood health. The association between childhood mortality and maternal education was not consistent with the expected pattern, since we ob- served no gradient between lower and higher educa- tion groups. However, there were nearly no women with no or only primary education in the sample and the difference between secondary and higher educa- tion may not influence childhood mortality.
We made the surprising observation that under-three mortality was lower in families with a large number of household members, although negative effects of lar-
OriginalArticle
Table 1: Demographic and socioeconomic characteristics of the study sample (in %)
ger households on children survival were postulated in the literature. However, larger household size was found to be associated with lower mortality in the analysis of cross-national variation in mortality predict- ors [15]. A possible explanation could be that the overall income in the household is higher and also more people can take care of the children. The nega- tive effect of the short length of the preceding birth in- terval on childhood mortality is well known [21]. As it was expected, our analysis showed lower mortality among children with the longer length of preceding birth interval (OR 0.61 (0.32-1.15)).
We found substantial country disparities in under-three mortality, namely children in Kyrgyzstan and Uzbe- kistan had a higher mortality compared to children liv-
ing in Kazakhstan as shown later this was mainly the case for the mortality in 2-36 months of life.
In many developing countries different studies found rural-urban differences in childhood mortality. Most of them showed higher mortality rates in rural than urban areas [4], [5]. In a multiple analysis after adjusting for parental education and some other socio-economic factors, the effect of the place of residence usually decreases [6]. In the simple logistic regression analysis we found higher under-three mortality in rural than urban areas (OR 1.64 (CI 1.11-2.41)). After controlling for other socio-economic factors in the multiple logistic regression analysis, the effect of the living place only slightly changed (OR 1.69 (CI 1.11-2.56)). It means that the effect of the living place was independent from
OriginalArticle
Table 2: Characteristics of the sample in relation to childhood mortality
other considered parameters like maternal education and may be more related to parameters like availability of health care [15].
Our analysis showed, that the risk of neonatal mortality was much higher in Kyrgyzstan and Uzbekistan com- pared to Kazakhstan. Kazakhstan was among the five former Soviet republics of Central Asia experiencing
OriginalArticle
Table 3: Characteristics associated with childhood mortality (simple and multiple logistic regression)
a better economic growth. Kazakhstan's gross national product per capita (GNP) was 1330 US$ in 1995, 1350 US$ in 1996 and 1340 US$ in 1997. The GNP per capita for Kyrgyzstan and Uzbekistan was estimated to be much lower (the GNP for Kyrgyzstan was 700 US$ in 1995, 550 US$ in 1996, 440 US$ in 1997 and for Uzbekistan 970 US$ in 1995, 1010 US$ in 1996, 1010 US$ in 1997) [22]. Some studies found higher neonatal mortality in countries with economic inequality [23], which can be assumed to be higher in the two countries with worse overall economic status (Kyrgyzstan, Uzbekistan). With nearly all children born in hospitals in the three countries, the neonatal mortal- ity may depend also on the equipment of hospitals which is mainly related to economic factors. Overall, the measures of the predictive power of the model in- dicated that the analyzed factors are more strongly associated with the mortality in 2-36 months of life than with neonatal mortality. In these characteristics
the countries were more similar, in opposition to the finding for neonatal mortality.
In conclusion, there is some indication that neonatal mortality can be improved by better socio-economic conditions on the country level. However in terms of under-three mortality all three Central Asian countries share the common characteristics associated with childhood mortality in developing countries.
Corresponding author:
• Dr. med. Rafael T. Mikolajczyk, School of Public Health, University of Bielefeld, PO-Box 100131, 33501 Bielefeld, Germany, Phone: +49 (0)521 106-6889, Fax: +49 (0)521 106-2968
rafael.mikolajczyk@uni-bielefeld.de
OriginalArticle
References:
[1] Veenema TG. Health Systems and Maternal and Child Survival in Central Asian Republics. Journal of Nursing Scholarship. 2000;32(3):301-6.
[2] Innocenti Social Monitor 2003. Available from:
http://www.unicef-icdc.org/publications/.
[3] Child Mortality in Developing Countries: Socio-economic Differentials, Trends and Implications. New York: United Nations; 1991.
[4] Defo B. Areal and socioeconomic differentials in infant and child mortality in Cameroon. Soc Sci Med.
1996;42(3):339-420.
[5] Sastry N. What explains rural-urban differentials in child mortality in Brazil? Soc Sci Med. 1997;44(7):989-1002.
[6] Trussel J, Preston S. Estimating the covariates of childhood mortality from retrospective reports of mothers.
Health Policy Educ. 1982;3(1):1-36.
[7] Kim TH. Changing determinants of infant and child mortality: on the basis of the Korean experience 1955-73. J Biosoc Sci. 1988;20(3):345-55.
[8] Madise NJ, Diamond I. Determinants of infant mortality in Malawi: an analysis to control for death clustering within families. J Biosoc Sci. 1995;27(1):95-106.
[9] Demographic and Health Surveys 2006. Available from:
http://www.measuredhs.com/.
[10] Demographic and Health Survey 1997. Kyrgyz Republic Final Report 2006. Available from:
http://www.measuredhs.com/pubs/search_results.cfm?
newSrch=1&srchTp=ctry&ctryid=21.
[11] Demographic and Health Survey 1995. Kazakhstan Final Report 2006. Available from:
http://www.measuredhs.com/pubs/pdftoc.cfm?ID=114.
[12] Demographic and Health Survey 1996. Uzbekistan Final Report 2006. Available from:
http://www.measuredhs.com/pubs/pdftoc.cfm?ID=126.
[13] Guo G. Use of sibling data to estimate family mortality effects in Guatemala. Demography. 1993;30(1):15-32.
[14] Basu AM, Stephenson R. Low levels of maternal education and the proximate determinants of childhood mortality: a little learning is not a dangerous thing. Soc Sci Med. 2005;60(9):2011-23.
[15] Heaton TB, Forste R, Hoffman JP, Flake D.
Cross-national variation in family influences on child health.
Soc Sci Med. 2005;60(1):97-108.
[16] Manda SOM. Birth intervals, breastfeeding and determinants of childhood mortality in Malawi. Soc Sci Med.
1999;48(3):301-12.
[17] Allison PD. Logistic regression using the SAS system:
theory and application. 2 ed. Cary, NC: SAS Institute; 2000.
[18] Steyerberg EW, Eijkemans MJ, Harrell FE, Jr., Habbema JD. Prognostic modelling with logistic regression analysis:
a comparison of selection and estimation methods in small data sets. Stat Med. 2000;19(8):1059-79.
[19] Hosmer DW, Lemeshow S. Applied logistic regression.
New York: Wiley; 2000.
[20] Yassin KM. Indices and sociodemographic determinants of childhood mortality in rural Upper Egypt. Soc Sci Med.
2000;51(2):185-97.
[21] Rutstein SO. Effects of preceding birth intervals on neonatal, infant and under-five years mortality and nutritional status in developing countries: evidence from the
demographic and health surveys. Int J Gyn & Obstetrics.
2005;89(Supplement 1):7-24.
[22] Progress of Nations. 2006. Available from http://www.unicef.org/publications.
[23] Mayer SE, Sarin A. Some mechanisms linking economic inequality and infant mortality. Soc Sci Med.
2005;60(3):439-55.
OriginalArticle