Hoffmann's syndrome: a case report
Hoffmann-Syndrom: ein Fallbericht
Abstract
This syndrome is characterized by the presence of hypothyroidism with myxoedema, muscle stiffness and pseudo hypertrophy. We describe
Waseem Qureshi
1Ghulam Hassan
2the disorder in a 21 year old male, who got admitted with complaints
Ghulam Qadir Khan
2of generalized weakness, cold intolerance, constipation, and hoarse
Syed Manzoor Kadri
3voice, difficulty in walking and progressive enlargement of muscles of thighs and back with crampy pains for two years. Examination revealed
Manish Kak
2mild mental retardation, enlarged tongue, dry and rough skin, enlarge-
Manzoor Ahmad
2ment of thighs and back muscles, motor weakness in flexors of hips
Shahid Tak
2and knees with delayed relaxation of deep tendon reflexes. Investiga- tions revealed evidence of hypothyroidism with marked elevation of
Darshan Lal Kundal
2muscle enzymes. Following institution of replacement therapy with
Showkat Hussain
2thyroxine, the patient showed marked clinical and biochemical improve-
Abdul Rashid Rather
2ments after six months, but insignificant decrease in muscle mass. In this report we review relevant literature.
Ibrahim Masoodi
2Keywords:hypothyroidism, myopathy, pseudohypertrophy
Sabia Sikander
2Zusammenfassung
Das Syndrom ist charakterisiert durch eine Hypothyreose mit Myxoedem, Pseudohypertrophie und Steifheit der Muskulatur. Das Syndrom wird
1 SMHS Hospital, Srinagar, Kashmir, India
2 Department of Medicine, Government Medical College, Srinagar, Kashmir, India beschrieben an einem 21-jährigen Patienten, der in die Klinik aufge-
nommen wurde wegen allgemeiner Schwäche, Kälteunverträglichkeit,
Obstipation, Änderung in der Stimmlage, Schwierigkeiten beim Gehen 3 Regional Institute of Health
& Family Welfare (RIHFW), bei gleichzeitiger Verdickung der Muskulatur an den Beinen und im
Rücken mit Muskelkrämpfen. Die Beschwerden bestanden seit zwei Directorate of Health Jahren. Die klinische Untersuchung ergab eine geringe geistige Retar- Services, Srinagar, Kashmir,
India dierung, eine vergrößerte Zunge, trockene und raue Haut, Hypertrophie
der Muskulatur an den Oberschenkeln und im Rücken, der Flexoren im Kniegelenk mit verlängerter Relaxation der tiefen Sehnenreflexe. Die Laboruntersuchungen ergaben Hinweise für eine Hypothyreose mit er- höhter Aktivität der Muskelenzyme. Nach Beginn der Substitutionsthe- rapie mit Thyroxin über sechs Monate zeigte der Patient deutlich ver- besserte klinische und biochemische Ergebnisse, aber nur einen gering- gradigen Rückgang der Muskelmasse. Die einschlägige Literatur wird in diesem Bericht besprochen.
Introduction
Hoffmann's syndrome, first described by Hoffmann in 1897, is characterized by the presence of hypothyroidism with muscle stiffness and pseudo hypertrophy. Whereas muscle hypertrophy with weakness and slowness of movement in cretinous children is known as Kocher Debre Semelaigne syndrome [1], [2], [3], [4], [5], [6], [7], [8], [9], [10]. However the two conditions tend to merge into each other and may even occur, although at different times in the same patient [3].The former in addition is characterized by few other clinical manifestations [6].
This syndrome is a very rare disorder. In India only few cases have been reported so far [2], [7], [8] and to our
knowledge the present case is the first case reported from the Jammu and Kashmir State.
Case presentation
A 21-year-old male of non consanguineous parents was admitted to our Department of Medicine, Government Medical College, Srinagar, Kashmir, India with complaints of generalized weakness, cold intolerance, enlargement of muscles of thighs and back and crampy pain in the calf and thigh muscles for the last two years. Further en- quiry revealed that he had constipation, hoarseness of voice and difficulty in walking of same duration. His de-
1/4 GMS German Medical Science 2005, Vol. 3, ISSN 1612-3174
Case Report
OPEN ACCESS
Figure 1: 21-year-old male patient with Hoffmann's syndrome
velopmental history and milestones were consistent with age. There was no history of swelling of or operation on the thyroid gland, any medication prior to the onset of illness or hospitalization for any significant illness in the past. None of the family members from maternal and paternal side suffered from such illness.
On examination he had dull look, mild mental retardation, hoarse voice, moderately enlarged tongue, dry and rough skin and visible enlargement of thigh and back (Figure 1). Thyroid was non-tender and not enlarged, a non-pitting edema was present at the pretibial sites. He appeared lethargic and his activities were slow. Pulse was slow (54 beats/min) regular, without any special character and all the peripheral pulses were palpable and synchronous.
Blood pressure was 100/60 mmHg. His body weight was 47 kg, height 151 cm and body mass index (BMI) was 20.6 kg/m2. Girth at the level of maximum enlargement of muscles of back was 96 cm, that of thigh muscles at the level of maximum enlargement was 49 cm on right and 46 cm on left side. Fundoscopic examination was normal. Genitalia and hair distribution were normal and there was no musculoskeletal deformity. His cardio- thoracic and abdominal examination was normal. On neurological examination he was mentally retarded, had grade 4 power of the flexors of hips and knees on both sides, biceps, ankles and knee reflexes had classical delayed relaxation. Investigations on admission revealed elevated serum levels of cholesterol of 320 mg/dl, aspart- ate aminotransferase (AST) 46 U/L (0-25 U/L), lactate dehydrogenase (LDH) 2432 U/L (100-190 U/L), creatinine phosphokinase (CPK) 763 U/L (25-90 U/L) and aldolase 14.5 U/L (0-6 U/L). Thyroid function testing revealed the serum levels of thyroid stimulating hormone (TSH) elev- ated to 9.2 µU/ml (0.4-5 µU/ml) and decreased levels of thyroxine (T4) of 3.2 µg/dl (5-12 µg/dl) and plasma triiodo- thyronine (T3) of 43.6 ng/dl (70-190 ng/dl). The electro- cardiogram was of low voltage having sinus bradycardia
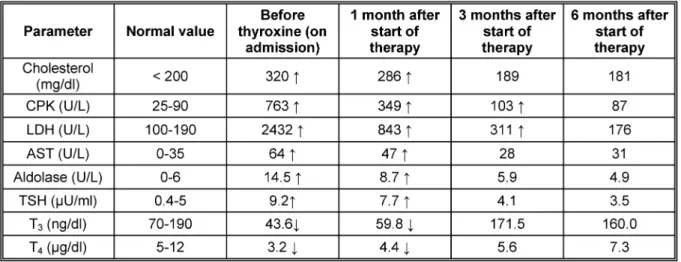
with rate of 52/min. Biopsy of thigh mucles taken at side of enlargement showed hypertrophy of muscle fibers with increased nuclei, few necrotic fibers and mucoid deposits at places and electromyography of hypertrophied muscles revealed complex repetitive discharges. Nerve conduction velocity studies were normal and ultrasonography of thyroid and detailed skeletal survey did not reveal any abnormality. All other hematological, biochemical, serolo- gical and endocrinological investigations performed in detail and repeatedly were normal. With the findings of hypothyroidism and muscle hypertrophy, the patient was put on replacement therapy with levothyroxine, started from 25 µg/d and increased to 100µg/d. After this the patient noticed improvement of his symptoms within four weeks. Repeated anthropometric measurements and investigations were performed over a period of six months (Table 1, Table 2). The patient showed marked improve- ment in symptomatology and biochemical parameters including muscle enzymes but there is no significant im- provement of muscle hypertrophy despite months of therapy.
Discussion
The present case got significant improvement of symp- toms like cold intolerance, weakness, constipation, hoarseness of voice, muscle cramps, weakness of flexors of hip and knee, pretibial edema, mentation and appear- ance of skin by three months of institution of thyroxine replacement and the various biochemical parameters returned to normal by 6 months. However, the enlarged muscle mass did not show any significant improvement, although body weight got reduced by 2 kg. The improve- ment in symptoms and biochemical abnormalities cured in a relatively long period of 3 to 6 months compared to previous studies were the significant improvement was
2/4 GMS German Medical Science 2005, Vol. 3, ISSN 1612-3174
Qureshi et al.: Hoffmann's syndrome
Table 1: Anthropometric measurements before and after thyroxine replacement
Table 2: Laboratory parameters before and after thyroxine replacement
observed in shorter period of 10 weeks to 3 months [1], [2], [4], [5], [8]. The insignificant improvement of muscle enlargement in our study is similar to that of Astrom et al. [11] where there was no response to thyroxine therapy for a prolonged period.
Muscular complaints are common symptoms of disorder and increased volume of muscle and slowness of contrac- tion constitute the muscular syndrome [1], [5], [6]. The entire musculature is affected to some extent but the most obvious enlargement is in the tongue, arms and legs. In one woman the biceps had become so thick that she could not touch her thumb and little finger [6].
Chopra et al. [8] noticed hypertrophy of almost all muscles of body, especially calf and arm muscles. In comparison to this we observed enlargement of tongue, thigh and spinal muscles. A sense of stiffness and even slight dis- comfort in the large muscles are frequent complaints and movements may even be mildly painful. These are prob- ably the expressions of the basic slowness of contraction [3], [5], [6]. Whether this slowness of contraction and relaxation is the same as myotonia, has been a subject of debate. The consensus is that it differs from myotonia and should therefore be called pseudomyotonia. Unlike
myotonia there is slowness of contraction and relaxation and slowness of the latter is not increased after rest or relieved by repeated contraction of the muscle. Further striking the muscle belly so called "percussion myotonia"
does not elicit a response in pseudomyotonia [6]. Kugel- berg (1959) reported 3 cases in whom there was no evidence of myotonia or hypertrophy but those cases proved to have myopathy by electromyographic and his- tological studies [2]. Muscle biopsies in most of the studies have revealed no abnormalities [1], [4], [6], [8].
The biopsy study in our case showed hypertrophy of muscle fibers with increased nuclei, few necrotic fibers and mucoid deposits at places and the findings are coin- ciding the studies of Mastropasqua [1] and Mishra [2]
The high level of CPK, LDH, AST and aldolase are indica- tive of muscle disorder and many studies of skeletal muscle have shown that changes in expression of the myosin heavy gene accompany thyroid states [1], [4]. It is known that hypothyroidism can lead to increase in CPK release from skeletal muscle, serum levels of CPK may be elevated in 70%-90% of hypothyroidism patients.
However no correlation has been found between CPK levels and circulating concentration of T3, T4 and thyro-
3/4 GMS German Medical Science 2005, Vol. 3, ISSN 1612-3174
Qureshi et al.: Hoffmann's syndrome
tropin. The presence of triiodothyronine receptor on the mitochondrial membrane of skeletal muscle suggests a direct impact of thyroid hormones on oxidative metabol- ism and may provide a biochemical basis for the muscle dysfunction in hypothyroidism. Even severe hypothyroid- ism may reduce glycolysis and oxidative phosphorylation and thus reduce adenosine triphosphate concentrations beyond a critical limit, generating a marked release of CPK through the altered sarcolemmal membrane [1].
Other less common associations of the disorder include peripheral neuropathy, facial weakness, cerebellar ataxia and dementia. Secondary sexual characteristics are not altered [1], [6]. The present case is having no such manifestation and is under our regular follow up for future course.
References
1. Mastropasqua M, Spagna G, Baldini V, Tedesco I, Paggi A.
Hoffman's syndrome: muscle stiffness, pseudohypertrophy and hypothyroidism. Horm Res. 2003;59(2):105-8.
2. Mishra SC, Mohanta KD, Bidyadhar S. Hoffmann's syndrome.
Indian J Med Sci. 1970;24(6):338-40.
3. Engel AG. Metabolic and endocrine myopathies. In: Walton J, ed.
Disorders of voluntary muscle. 5. ed. Edinburgh [u.a.]: Churchill Livingstone; 1988. p. 811-68.
4. Cronstedt J, Carling L, Ostberg H. Hypothyroidism with subacute pseudomyotonia--an early form of Hoffmann's syndrome? Report of a case. Acta Med Scand. 1975;198(1-2):137-9.
5. Klein I, Parker M, Shebert R, Ayyar DR, Levey GS. Hypothyroidism presenting as muscle stiffness and pseudohypertrophy:
Hoffmann's syndrome. Am J Med. 1981;70(4):891-4.
6. Adams RD, Rosman NP. Neuromuscular System. In: Werner SC, Ingbar SH, eds. The thyroid; a fundamental and clinical text. 3rd ed. New York: Harper & Row; 1971. p. 771-80.
7. Omer S. Hoffmann's syndrome (Hypothyroid myopathy). J Assoc Physicians India. 1964;12:353-8.
8. Chopra BK, Singh G, Puri A. Hoffman's Syndrome (hypothyroid Myopathy). J Assoc Physicians India. 1972;20(5):387-90.
9. Sidibe EH, Diop AN, Thiam A, Diagne PM, Sarr A, Toure M, Diop M. Hoffmann's syndrome in hypothyroid myopathy. Report of a case in an African. Joint Bone Spine. 2001;68(1):84-5.
10. Kasperek S, Biernawska J, Kurzbauer H. Zespol Hoffmanna.
Udzial neurologa w wykrywaniu niedoczynnosci tarczycy.
[Hoffmann's syndrome. The role of neurologists in the diagnosis of hypothyroidism]. Neurol Neurochir Pol. 1989;23(1):64-7.
11. Astrom KE, Kugelberg E, Muller R. Hypothyroid myopathy. Arch Neurol. 1961;5:472-82.
Erratum
The name of the co-author Ibrahim Masoodi was first er- roneously indicated as Mohammad Ibrahim.
Corresponding author:
Ghulam Qadir Khan
PO Box 1143, GPO, Srinagar 190001, Kashmir, India kadrism@sancharnet.in
Please cite as
Qureshi W, Hassan G, Khan GQ, Kadri SM, Kak M, Ahmad M, Tak S, Kundal DL, Hussain S, Rather AR, Masoodi I, Sikander S. Hoffmann's syndrome: a case report. GMS Ger Med Sci. 2005;3:Doc05.
This article is freely available from
http://www.egms.de/en/journals/gms/2005-3/000023.shtml
Received:2005-03-24 Published:2005-07-20
Published with erratum:2010-09-09
Copyright
©2005 Qureshi et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by-nc-nd/3.0/deed.en). You are free: to Share — to copy, distribute and transmit the work, provided the original author and source are credited.
4/4 GMS German Medical Science 2005, Vol. 3, ISSN 1612-3174
Qureshi et al.: Hoffmann's syndrome