Quality of life following surgery for congenital or acquired trigger finger
Untersuchung der Lebensqualität nach chirurgischer Versorgung der angeborenen und erworbenen Ringbandstenose
Abstract
Background:Evaluation of quality of life following surgical release of the first annular flexor tendon pulley in children suffering from pediatric trigger thumb in comparison to adult patients with trigger finger.
Heiko Sorg
1Robert Krämer
1Julia M. Reinke
1Material and methods:All patients who underwent an A1 tendon pulley
release between 2006 and 2010 at a hand surgery center were re-
Ludwik K. Branski
1viewed retrospectively. Chart review included operation type, length of
Karsten Knobloch
2hospital stay, and type of anesthesia. Patient satisfaction was assessed using two validated hand questionnaires, the Disabilities of the Arm, Shoulder and Hand (DASH) Outcome Measure and the German Michigan Hand Outcomes Questionnaire (MHQ).
1 Department of Plastic, Hand and Reconstructive Surgery, Hannover Medical School, Hannover, Germany Results: A total of 13 children and 147 adults were included in the
study. No postoperative complications or recurrence were observed in
the pediatric patient population. Postoperative DASH score in children 2 SportPraxis Prof. Dr. med.
Karsten Knobloch, Hannover, Germany
was 0±0 and in adults 14±2. Postoperative German MHQ score was 97±3 in children and 84±2 in adults. Patient satisfaction was rated positive in all children and in 87% of adults; all children and 93% of the adults would undergo this procedure again.
Conclusions:The surgical release of the A1 pulley in children and adults is a safe and low-risk procedure. Postoperative quality of life, especially in children, is high; patients and parents were highly satisfied. Therefore, the surgical approach should be recommended as a first-line treatment of the trigger finger in all age groups.
Keywords:pediatric trigger thumb, open release, DASH, German MHQ
Zusammenfassung
Hintergrund: Evaluation der Lebensqualität nach chirurgischer Ring- bandspaltung bei angeborener Ringbandstenose des Daumens bei Kindern (Pollex flexus congenitus) sowie erworbener Ringbandstenose bei Erwachsenen.
Material und Methoden:Retrospektiv wurden allgemeine Patientendaten nach offener Ringbandspaltung zwischen 2006 und 2010 sowie die Patientenzufriedenheit mit den Patienten-orientierten Fragebögen Mi- chigan Hand Outcomes Questionnaire (MHQ) und Disabilities of the Arm, Shoulder and Hand (DASH) Outcome Measure ausgewertet und analysiert.
Ergebnisse:13 Kinder und 147 erwachsene Patienten wurden in die Studie aufgenommen. Postoperativ kam es bei den Kindern zu keinen Komplikationen oder dem Wiederauftreten eines Schnappphänomens des Daumens. Der postoperative DASH-Score der Kinder war 0±0 Punkte und bei den Erwachsenen 14±2. Der postoperative MHQ- Score lag bei den Kindern bei 97±3 Punkten, der der Erwachsenen bei 84±2. Die postoperative Zufriedenheit wurde bei allen Kindern und bei 87% der erwachsenen Patienten als positiv gewertet. Alle Kinder sowie 93% der Erwachsenen würden sich erneut diesem operativen Eingriff unterziehen.
Schlussfolgerung: Die chirurgische Intervention zur Behandlung des Pollex flexus congenitus bei Kindern sowie der Ringbandstenose bei Erwachsenen ist ein sicherer und risikoarmer Eingriff. Die postoperative Lebensqualität, speziell die der Kinder, ist hoch. Daher kann das chirur- gische Vorgehen als First-Line-Therapie beim schnellenden Finger in allen Altersgruppen empfohlen werden.
Schlüsselwörter:Pollex flexus congenitus, offene Spaltung, DASH, German MHQ
Introduction
The measurement of quality of life following surgical procedures of the hand is an evolving field. Beyond the functional aspect, issues such as daily activities and their impairment may play a substantial role for the individual affected by a hand disorder. The pediatric trigger thumb usually presents between six months and two years of age. The interphalangeal joint of the thumb is usually locked in flexion with a palpable A1 pulley known as the Notta node [1]. While mild cases do not warrant any therapy at all, steroid injections have not been accepted in this patient cohort [2]. Spontaneous resolution of pedi- atric trigger thumbs are observed in 12–75% of patients [3], [4], [5], [6], [7]. Surgical release of the A1 pulley is believed to be almost always successful [8], [9], [10], however to date, no follow-up data on quality of life has been published.
The trigger finger in the adult, also known as stenosing tenosynovitis, is a frequent hand disorder caused by a disparity in size between the flexor tendon and the sur- rounding retinacular pulley system (tendon sheath).
Consecutively, the affected flexor tendon cannot glide freely and causes intermittent pain and snapping [11].
The lifetime incidence of trigger finger is 2% [12]. Another study estimates that 28 in 100,000 persons are suffering from trigger finger [13]. According to the guidelines of the British Society of Surgery of the Hand (BSSH), steroid in- jection is an effective therapy for trigger finger therapy with success rates varying between 49–78%. Surgery, according to the aforementioned guideline, is recommend- ed after failed conservative treatment, for recurrent trig- gering after 1–2 injections of steroids, if there are severe symptoms at time of presentation, or in people who are unlikely to benefit from steroid injections [13].
We therefore sought to evaluate the quality of life follow- ing surgical release of the A1 pulley among children suf- fering from pediatric trigger thumb as well as in adult patients with trigger finger.
Material and methods
The study was designed as a retrospective study that in- cluded hospital chart review and patient-reported out- come assessment using the German version of the Dis- abilities of the Arm, Shoulder and Hand (DASH) Outcome
Measure [14], [15], [16] and the validated German Michigan Hand Questionnaire (MHQ) [17].
Chart review
Subjects were identified through a computerized search by ICD-10 code (M65.3) for all patients undergoing sur- gery for trigger thumbs or trigger fingers in both children and adults at our department between January 1, 2006, and December 31, 2010. Data collected included age, gender, status of surgeon (resident/consultant), method of anesthesia, and postoperative symptoms or complica- tions.
Outcome measure tools – DASH and German MHQ
The Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire is an outcomes data collection instrument using a 30-item disability/symptom scale measuring components of the patient’s health-status relevant to upper-extremity conditions during the preceding week.
Using the questionnaire as a self-report system, patients attribute the degree of difficulty in performing different physical activities because of problems at the arm, shoulder, or hand (21 items); the severity of each of the symptoms of pain, activity-related pain, tingling, weak- ness, and stiffness (5 items); as well as the problem’s impact on social activities, work, sleep, and self-image (4 items). Items are answered on 5-point Likert scales.
The raw score is then transformed to a score from 0 (no disability) to 100 (most severe disability). The score for the disability/symptom scale is called the DASH score.
The German version of the DASH questionnaire has been previously standardized and validated [14], [15], [16].
The Michigan Hand Outcomes Questionnaire (MHQ) has also been developed as a hand specific outcomes tool applying psychometric principles to create an instrument measuring the health status of patients with hand or wrist disorders. The questionnaire consists of 37 core ques- tions with 5-point scales evaluating the overall hand function, activities of daily living, pain, work performance, aesthetics, and patient satisfaction with the overall hand function. A demographic section at the end of the ques- tionnaire asks about the patients’ age, the ethnic back- ground, and the socioeconomic status. The raw scale score is the sum of responses to each scale item, which is then converted to a score ranging from 0 (worst hand
performance) to 100 (best hand performance). The Ger- man version of the MHQ questionnaire (MHQ) has been standardized and validated by our own group [17].
The DASH Outcome Measure and the German MHQ have been accompanied by further questions about postopera- tive satisfaction, numeric rating scale (NRS) for pain evaluation, and respective corticosteroid therapy before surgery. In pediatric patients, parents filled out the re- spective questionnaires for their children. The primary endpoints of this study have been defined as the scoring values of the DASH and German MHQ questionnaires.
Surgical procedure
The surgical procedure to release the A1 pulley was per- formed in local or general anesthesia and in loco-regional Esmarch ischemia. A transverse incision was performed on the palmar aspect of the hand overlying the MCP joint and A1 pulley or the transverse flexor fold at the MCP joint of the thumb in children, respectively. Neurovascular structures were identified by blunt dissection down to the flexor tendon visualizing the A1 pulley. After correct identification the pulley was dissected completely, fol- lowed by traction on the flexor tendon proximal to the A1 to exclude persistent triggering or locking of the respective finger. After meticoulus hemostasis, the skin was closed using absorbable sutures in children and non-absorbable sutures in adults; in the latter, sutures were removed 10–12 days postoperatively. The surgical procedure was finished by application of a bulky soft dressing. An early postoperative exercise regimen was applied in all patients after wound healing was complete.
Results
Demographic data
A total of 160 patients were operated on between 2006 and 2010 and were invited to participate. The study sample comprised 13 children (7 girls; 6 boys) and 147 adult patients (87 women; 50 men). The mean age of the children was 5±3 years, that of adult patients was 61±14 years. The chart review data presented in this study were obtained from this entire cohort. A total of 73 patients responded to our invitation and filled out the DASH and German MHQ questionnaires. Mean follow-up time in adults has been 33±1 months and in children 33±3 months postoperatively.
General patient characteristics
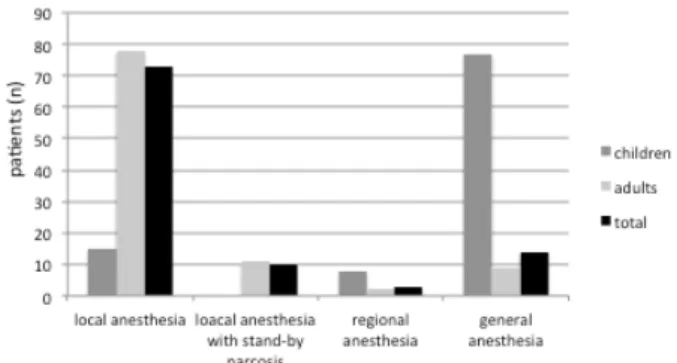
Most of the children were operated under general anes- thesia (77%). A brachial plexus block was used in 8% and local anesthesia in 15% of the pediatric patients (Figure 1). In adult patients, these ratios were reversed, with most of the adult patients operated in local anes- thesia (78%), and only 9% operated under general anes- thesia and only 2% with a regional anesthesia (Figure 1).
Six adult patients (4%) received preoperative steroid treatment with an average of 2±1 injections, but only half of them had a profit by this treatment of more than a month. Surgery has been performed as an outpatient surgery in 82% of adults but only in 23% of the children.
Here, most children have been admitted to the ward (77%) for postoperative monitoring. Mean operating time was 17±2 min in children and 19±1 min in adults. 85%
of the children and 93% of the adult patients have been operated by a consultant. Patient satisfaction with the operative procedure was rated positive in all pediatric patients and in 87% of adults. All children and 93% of the adults would undergo this procedure again (Figure 2).
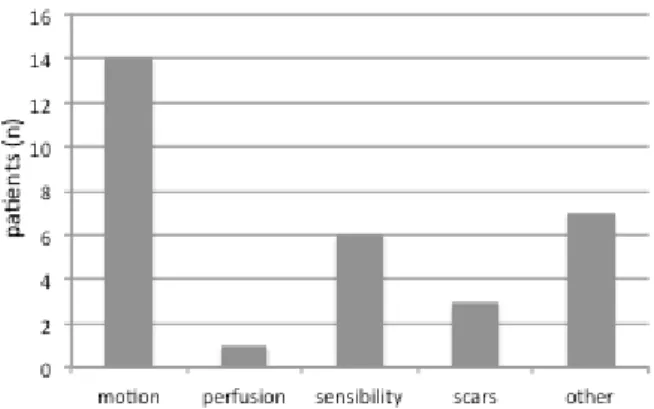
Postoperative complications were reported by 21% of all adult patients (Figure 3). Furthermore, only adult patients reported post-operative pain, with values reaching an average of 0.7/10 numeric rating scale (NRS; resting) and 1.4/10 NRS (stress).
Figure 1: Total numbers of the chosen forms of anesthesia for the surgical release of trigger thumbs (children) and trigger
fingers (adults)
Figure 2: Satisfaction of patients with surgery and their disposition to perform the respective procedure again
Figure 3: Total numbers of reported postsurgical patient complications after surgical release of the A1 pulley in a total
of 73 adult patients
Postoperative DASH score
In children, the mean DASH score was 0±0 and in adults 14±2 (95% confidence interval (CI) 15–12, Figure 4A);
subscores of adult DASH were DASH work 11±3 (95% CI 12–9) and DASH sport 15±4 (95% CI 17–13).
Figure 4: Box plot diagrams of the mean total scores of the DASH Outcome Masure (A) and the German MHQ (B) of children and of adults after surgical release of the A1 pulley for trigger
thumbs in children and trigger fingers in adults
Postoperative German MHQ score
In children, the mean German MHQ score was 97±3 (95%
CI 99–95) and in adults 84±2 (95% CI 85–82, Figure 4B).
German MHQ subscores for adults were 84±3 (95% CI 85–82) for the German MHQ work and 20±3 (95% CI 22–18) for the German MHQ pain.
Discussion
The main rationale of this study was to assess the quality of life following surgical release of a trigger thumb in children in comparison to trigger fingers in adult patients.
The current literature lacks sufficient data from random- ized studies or case reports. To the best of our knowledge, this is the first quantitative and standardized analysis of postoperative outcome measures after trigger finger re- lease using two validated questionnaires for hand dis- orders (DASH, German MHQ) in children and in adult pa- tients.
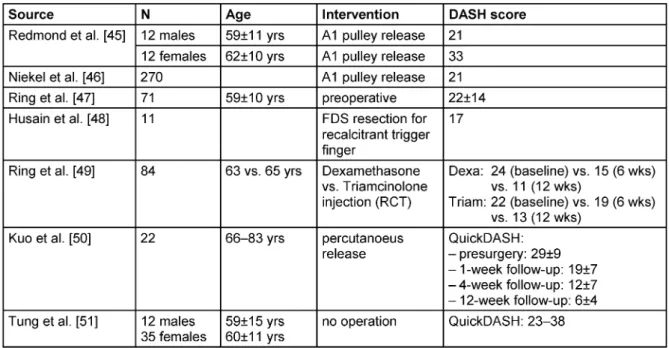
One of the major findings is that children present with excellent postoperative results represented by very good DASH and German MHQ scores, implying the highest levels of quality of life after surgery for trigger finger re- lease. No recurrence of triggering or nodules and no re- ported functional deficit of the thumb were found in the pediatric cohort. Furthermore, children and their parents were highly satisfied with the treatment. It can therefore be concluded that the surgical procedure is a safe and low-risk method to restore the physiological function of the thumb [18]. In the adult cohort, low DASH and high German MHQ scores represent a similarly outstanding functional outcome. Compared to other publications, the adult DASH score results in this study are in the top third of reported outcomes (mean DASH between 11 and 33 points; Table 1). However, in comparison to other hand related diseases, i.e. Dupuytren disease, de Quervain’s tenosynovitis, and cubital tunnel syndrome, patients suffering from trigger digits are suffering much less, mostly caused by a lesser degree of nerval damage.
In many centers, patients undergo a corticosteroid injec- tion prior to surgery, which is also described as the first- line treatment [19], [20], [21]. Longterm results, however, are largely missing. Another meta-analysis concluded that the percutaneous release of trigger fingers has similar efficacy to open surgical release and is superior to steroid injection [22]. In our entire patient cohort of adult pa- tients, the injection of corticosteroids has only been per- formed in 4% of the patients, and a satisfying effect was only achieved in half of those injected at least two times.
Furthermore, even when treated with corticosteroid injec- tion, eventually all of those patients decided to undergo surgery. The corticosteroid injection in children seems not to be the primary choice of treatment [3], [23], [24], [25], although a study by Pechora in 1985 showed satis- factory results in children under the age of three with an initial stage of trigger thumb [2].
Table 1: Overview of the studies using the disabilities of the arm, shoulder and hand (DASH) questionnaire for the assessment of the function of trigger finger patients and respective treatment alternatives
In contrast to a clear preference for a surgical approach in adults, in children the indication for surgery is not clear cut. A large body of literature recommending a primary surgical therapy [3], [26], [27], [28], [29], [30], [31] is matched by an equally large amount of studies and ob- servations which suggest a conservative treatment with a delay or even complete avoidance of surgery [3], [4], [5], [6], [7]. Additionally, there is no clear answer to the question which surgical approach might be the best. While Fuentes and colleagues recommend the percutaneous approach to release the A1 pulley [32], Ramirez et al.
recommend open surgery, due to the high rate of recur- rences after percutaneous release [33]. However, in all cases of failed conservative treatment, painful triggering, or for those with severe hyperextension deformity of the MCP joint of the thumb, surgical release (open or percu- taneous) seems to be the standard procedure [23], [30], [33], [34], [35], [36]. In these cases, it is recommended for the open release to be performed within the first 6 to 12 months after birth, latest at the age of 3 years [3], [23]. In patients younger than three years, the surgery is based on the release of the A1 pulley only. Later on, in children older than three years, different contractures might additionally be released in the course of the flexor tendon. This, however, could also be done with good post- operative results, implying that the age does not affect the outcome [3], [30], [34], [37], [38]. While adult pa- tients choose local anesthesia for this surgical procedure by approximately 80%, the method of anesthesia in chil- dren is dependent on the age as well as on the tolerance of the child and its parents. Here, it is reported that this operation can easily be done in children between 2 to 2.5 years, while younger children cannot hold still for the surgical procedure and older ones have great fear [35].
Commonly, the pressure of financial budgets and the
good possibility to perform this procedure in local anes- thesia could be the basis for further debate on this topic.
The hand questionnaires used in this study are reliable and validated instruments to evaluate hand disease re- lated outcomes [14], [15], [16], [39], and can also be used for the evaluation of trigger finger patients. The study design of a cohort study might be associated with a lower level of evidence; it is however, more feasible and sufficiently strong to draw the respective conclusions [40]. One potential limitation of this study may also be the use of the DASH Outcome Measure and the German MHQ for children. However, a standardized and validated questionnaire for the evaluation of the surgical outcome and quality of life of hand disorders in children does not exist [41], [42], [43], [44]. Nevertheless, this form has been used to study the outcome of the above-mentioned question with good results, even when children were not able to answer every question. It has been reported that the DASH score is valid even if 10 percent of the items are left blank (http://dash.iwh.on.ca/). Similarly, this is true for the MHQ, where even up to 25% can be missing from one scale (http://sitemaker.umich.edu).
Conclusion
In summary, the surgical approach for treatment of trigger thumbs in children and trigger fingers in adults is a safe and low-risk procedure, which is associated with a high postoperative quality of life, especially in children. A controversy about the correct approach in children, however, still exists, and a clear and evidence-based strategy cannot be described. Clearly, longitudinal pro- spective studies are needed to solve the question which therapy option is associated with the best short and long- term outcome.
Notes
Competing interests
The authors declare that they have no competing in- terests.
Authorship
Heiko Sorg and Robert Krämer contributed equally.
References
1. Clapham PJ, Chung KC. A historical perspective of the Notta’s node in trigger fingers. J Hand Surg Am. 2009 Oct;34(8):1518- 22. DOI: 10.1016/j.jhsa.2009.04.041
2. Pechora TA. Primenenie gidrokortizona pri lechenii stenoziruiushchego ligamentita pal’tsev kisti u detei [Use of hydrocortisone in treating stenotic tendovaginitis of the fingers in children]. Vestn Khir Im I I Grek. 1985 Apr;134(4):97-9.
3. Ger E, Kupcha P, Ger D. The management of trigger thumb in children. J Hand Surg Am. 1991 Sep;16(5):944-7.
4. Baek GH, Lee HJ. The natural history of pediatric trigger thumb:
a study with a minimum of five years follow-up. Clin Orthop Surg.
2011 Jun;3(2):157-9. DOI: 10.4055/cios.2011.3.2.157 5. Dinham JM, Meggitt BF. Trigger thumbs in children. A review of
the natural history and indications for treatment in 105 patients.
J Bone Joint Surg Br. 1974 Feb;56(1):153-5.
6. Fahey JJ, Bollinger JA. Trigger-finger in adults and children. J Bone Joint Surg Am. 1954 Dec;36-A(6):1200-18.
7. Baek GH, Kim JH, Chung MS, Kang SB, Lee YH, Gong HS. The natural history of pediatric trigger thumb. J Bone Joint Surg Am.
2008 May;90(5):980-5. DOI: 10.2106/JBJS.G.00296 8. Bae DS. Pediatric trigger thumb. J Hand Surg Am. 2008
Sep;33(7):1189-91. DOI: 10.1016/j.jhsa.2008.04.017 9. Ogino T. Trigger thumb in children: current recommendations for
treatment. J Hand Surg Am. 2008 Jul-Aug;33(6):982-4. DOI:
10.1016/j.jhsa.2008.05.006
10. British Society for Surgery of the Hand. BSSH Evidence for Surgical Treatment 1. Trigger Finger (Thumb). 2010.
11. Makkouk AH, Oetgen ME, Swigart CR, Dodds SD. Trigger finger:
etiology, evaluation, and treatment. Curr Rev Musculoskelet Med.
2008 Jun;1(2):92-6. DOI: 10.1007/s12178-007-9012-1 12. Moore JS. Flexor tendon entrapment of the digits (trigger finger
and trigger thumb). J Occup Environ Med. 2000 May;42(5):526- 45. DOI: 10.1097/00043764-200005000-00012
13. Akhtar S, Bradley MJ, Quinton DN, Burke FD. Management and referral for trigger finger/thumb. BMJ. 2005 Jul;331(7507):30- 3. DOI: 10.1136/bmj.331.7507.30
14. Germann G, Harth A, Wind G, Demir E. Standardisierung und Validierung der deutschen Version 2.0 des „Disability of Arm, Shoulder, Hand“ (DASH)-Fragebogens zur Outcome-Messung an der oberen Extremität [Standardisation and validation of the German version 2.0 of the Disability of Arm, Shoulder, Hand (DASH) questionnaire]. Unfallchirurg. 2003 Jan;106(1):13-9.
DOI: 10.1007/s00113-002-0456-x
15. Germann G, Wind G, Harth A. Der DASH-Fragebogen – Ein neues Instrument zur Beurteilung von Behandlungsergebnissen an der oberen Extremität [The DASH (Disability of Arm-Shoulder-Hand) Questionnaire – a new instrument for evaluating upper extremity treatment outcome]. Handchir Mikrochir Plast Chir. 1999 May;31(3):149-52. DOI: 10.1055/s-1999-13902
16. Offenbächer M, Ewert T, Sangha O, Stucki G. Validation of a German version of the ‘Disabilities of Arm, Shoulder and Hand’
questionnaire (DASH-G). Z Rheumatol. 2003 Apr;62(2):168-77.
DOI: 10.1007/s00393-003-0461-7
17. Knobloch K, Kuehn M, Papst S, Kraemer R, Vogt PM. German standardized translation of the michigan hand outcomes questionnaire for patient-related outcome measurement in Dupuytren disease. Plast Reconstr Surg. 2011 Jul;128(1):39e- 40e. DOI: 10.1097/PRS.0b013e318218fd70
18. Marek DJ, Fitoussi F, Bohn DC, Van Heest AE. Surgical release of the pediatric trigger thumb. J Hand Surg Am. 2011 Apr;36(4):647-652.e2. DOI: 10.1016/j.jhsa.2011.01.011 19. Nimigan AS, Ross DC, Gan BS. Steroid injections in the
management of trigger fingers. Am J Phys Med Rehabil. 2006 Jan;85(1):36-43.
20. Lambert MA, Morton RJ, Sloan JP. Controlled study of the use of local steroid injection in the treatment of trigger finger and thumb.
J Hand Surg Br. 1992 Feb;17(1):69-70. DOI: 10.1016/0266- 7681(92)90014-S
21. Murphy D, Failla JM, Koniuch MP. Steroid versus placebo injection for trigger finger. J Hand Surg Am. 1995 Jul;20(4):628-31. DOI:
10.1016/S0363-5023(05)80280-1
22. Izadpanah A, Kanevsky J, Izadpanah A, Shafran V, Shararah A, Luc M, Zadeh T. Treatment Modalities for Stenosing
Tenosynovitis: A Systematic Review and Meta-Analysis [Abstract].
Plastic Surgery The Meeting; 2011 September 23-27; Denver, Colorado. Available from: https://confex-
recordings.s3.amazonaws.com/asps/2011am/paper19518_2.pdf 23. Hierner R, Berger A. Tendovaginitis stenosans des Daumens
beim Kleinkind (Pollex flexus congenitus). Eigene Ergebnisse und Literaturübersicht. Chirurg. 1997;68(11):1190–3. DOI:
10.1007/s001040050344
24. Cardon LJ, Ezaki M, Carter PR. Trigger finger in children. J Hand Surg Am. 1999 Nov;24(6):1156-61. DOI:
10.1053/jhsu.1999.1156
25. Blauth W. Der Pollex flexus congenitus. Oper Orthop Traumatol.
1991;3(4):293-7. DOI: 10.1007/BF02513465
26. Dunsmuir RA, Sherlock DA. The outcome of treatment of trigger thumb in children. J Bone Joint Surg Br. 2000 Jul;82(5):736-8.
DOI: 10.1302/0301-620X.82B5.10250
27. Mulpruek P, Prichasuk S. Spontaneous recovery of trigger thumbs in children. J Hand Surg Br. 1998 Apr;23(2):255-7. DOI:
10.1016/S0266-7681(98)80190-3
28. Tan AH, Lam KS, Lee EH. The treatment outcome of trigger thumb in children. J Pediatr Orthop B. 2002 Jul;11(3):256-9.
29. McAdams TR, Moneim MS, Omer GE Jr,. Long-term follow-up of surgical release of the A(1) pulley in childhood trigger thumb. J Pediatr Orthop. 2002 Jan-Feb;22(1):41-3. DOI:
10.1097/01241398-200201000-00010
30. Skov O, Bach A, Hammer A. Trigger thumbs in children: a follow- up study of 37 children below 15 years of age. J Hand Surg Br.
1990 Nov;15(4):466-7. DOI: 10.1016/0266-7681(90)90092-I 31. van Loveren M, van der Biezen JJ. The congenital trigger thumb:
is release of the first annular pulley alone sufficient to resolve the triggering? Ann Plast Surg. 2007 Mar;58(3):335-7. DOI:
10.1097/01.sap.0000238336.30617.72
32. Marcos Fuentes L, Downey Carmona FJ, Tatay Díaz A, Macías Moreno E, Farrington Rueda D. Trigger thumb in children:
comparison of results between percutaneous release and open surgery. Rev Esp Cir Ortop Traumatol. 2010;54(6):351–6. DOI:
10.1016/S1988-8856(10)70261-3
33. Ramírez-Barragán A, Martínez-Caballero I, Epeldegui-Torre T.
Open Versus Percutaneous Surgery for Trigger Thumb in Children.
Rev Ortop Traumatol (Madr.). 2007;51(1):25–29.
34. Mulpruek P, Prichasuk S, Orapin S. Trigger finger in children. J Pediatr Orthop. 1998 Mar-Apr;18(2):239-41. DOI:
10.1097/01241398-199803000-00020
35. Wang HC, Lin GT. Percutaneous release for trigger thumb in children under general and local anesthesia. Kaohsiung J Med Sci. 2004 Nov;20(11):546-51. DOI: 10.1016/S1607- 551X(09)70256-6
36. Wang HC, Lin GT. Retrospective study of open versus
percutaneous surgery for trigger thumb in children. Plast Reconstr Surg. 2005 Jun;115(7):1963-70. DOI:
10.1097/01.PRS.0000165068.57709.4A
37. Schaverien MV, Godwin Y. Paediatric trigger finger: Literature review and management algorithm. J Plast Reconstr Aesthet Surg. 2011 May;64(5):623-31. DOI:
10.1016/j.bjps.2010.09.011
38. Moon WN, Suh SW, Kim IC. Trigger digits in children. J Hand Surg Br. 2001 Feb;26(1):11-2. DOI: 10.1054/jhsb.2000.0417 39. Changulani M, Okonkwo U, Keswani T, Kalairajah Y. Outcome
evaluation measures for wrist and hand: which one to choose?
Int Orthop. 2008 Feb;32(1):1-6. DOI: 10.1007/s00264-007- 0368-z
40. Graham B. Strategies for nonrandomized clinical research in hand surgery. Clin Plast Surg. 2005 Oct;32(4):529-36, vi-vii. DOI:
10.1016/j.cps.2005.06.001
41. Wood VE, Sicilia M. Congenital trigger digit. Clin Orthop Relat Res. 1992 Dec;(285):205-9.
42. Chien CW, Brown T, McDonald R. Examining content validity and reliability of the Assessment of Children’s Hand Skills (ACHS): a preliminary study. Am J Occup Ther. 2010 Sep-Oct;64(5):756- 67. DOI: 10.5014/ajot.2010.08158
43. Ho ES, Clarke HM. Functional evaluation in children with congenital upper extremity malformations. Clin Plast Surg. 2005 Oct;32(4):471-83, v. DOI: 10.1016/j.cps.2005.05.006 44. Chien CW, Brown T, McDonald R. Cross-cultural validity of a
naturalistic observational assessment of children's hand skills:
a study using Rasch analysis. J Rehabil Med. 2011 Jun;43(7):631-7. DOI: 10.2340/16501977-0827
45. Redmond CL, Bain GI, Laslett LL, McNeil JD. Hand syndromes associated with diabetes: impairments and obesity predict disability. J Rheumatol. 2009 Dec;36(12):2766-71. DOI:
10.3899/jrheum.090239
46. Niekel MC, Lindenhovius AL, Watson JB, Vranceanu AM, Ring D.
Correlation of DASH and QuickDASH with measures of psychological distress. J Hand Surg Am. 2009 Oct;34(8):1499- 505. DOI: 10.1016/j.jhsa.2009.05.016
47. Ring D, Kadzielski J, Fabian L, Zurakowski D, Malhotra LR, Jupiter JB. Self-reported upper extremity health status correlates with depression. J Bone Joint Surg Am. 2006 Sep;88(9):1983-8. DOI:
10.2106/JBJS.E.00932
48. Husain SN, Clarke SE, Buterbaugh GA, Imbriglia JE. Recalcitrant trigger finger managed with flexor digitorum superficialis resection. Am J Orthop. 2011 Dec;40(12):620-4.
49. Ring D, Lozano-Calderón S, Shin R, Bastian P, Mudgal C, Jupiter J. A prospective randomized controlled trial of injection of dexamethasone versus triamcinolone for idiopathic trigger finger.
J Hand Surg Am. 2008 Apr;33(4):516-22; discussion 523-4. DOI:
10.1016/j.jhsa.2008.01.001
50. Kuo LC, Su FC, Tung WL, Lai KY, Jou IM. Kinematical and functional improvements of trigger digits after sonographically assisted percutaneous release of the A1 pulley. J Orthop Res.
2009 Jul;27(7):891-6. DOI: 10.1002/jor.20825
51. Tung WL, Kuo LC, Lai KY, Jou IM, Sun YN, Su FC. Quantitative evidence of kinematics and functional differences in different graded trigger fingers. Clin Biomech (Bristol, Avon). 2010 Jul;25(6):535-40. DOI: 10.1016/j.clinbiomech.2010.02.009
Corresponding author:
Heiko Sorg, M. D.
Department of Plastic, Hand and Reconstructive Surgery, Hannover Medical School, Carl-Neuberg-Str. 1, 30625 Hannover, Germany, Phone: +49-511-532-0, Fax:
+49-511-532-8890
Sorg.Heiko@mh-hannover.de
Please cite as
Sorg H, Krämer R, Reinke JM, Branski LK, Knobloch K. Quality of life following surgery for congenital or acquired trigger finger. GMS Ger Plast Reconstr Aesthet Surg. 2015;5:Doc02.
DOI: 10.3205/gpras000030, URN: urn:nbn:de:0183-gpras0000301
This article is freely available from
http://www.egms.de/en/journals/gpras/2015-5/gpras000030.shtml Published:2015-03-02
Copyright
©2015 Sorg et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 License. See license information at http://creativecommons.org/licenses/by/4.0/.